info@biz4group.com
info@biz4group.com 




































Imagine a digital system that doesn’t wait for instructions but instead, understands your business goals, learns from real-time feedback, and takes independent actions to get the job done.
Read More

If over 90% of U.S. hospitals already operate with FHIR-enabled infrastructure, why do so many mental health platforms still struggle with EHR integrations?
Reports suggest that more than 90% of U.S. hospitals now operate with some level of FHIR-enabled infrastructure, increasing pressure on healthcare technology companies to support modern interoperability standards faster than ever before.
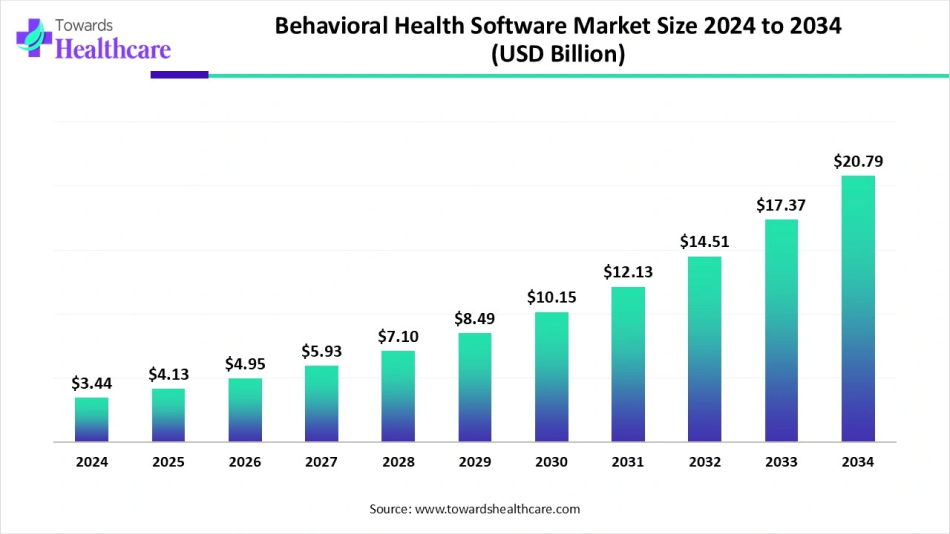
At the same time, behavioral health technology investments continue accelerating. The behavioral health software market is projected to grow from approximately $4.13 billion in 2025 to more than $20 billion by 2034, driven by rising demand for connected care ecosystems, digital behavioral health services, and enterprise-ready healthcare infrastructure.
So, here's the bigger question:
If healthcare organizations are rapidly adopting interoperable systems, why are so many teams still struggling with EHR integration for mental health platforms?
Because most teams underestimate what they're actually building.
You may think you're building therapy workflows, assessments, telehealth capabilities, clinician dashboards, patient engagement features, or behavioral health automation.
Then your first enterprise conversation happens.
A hospital asks: "Can your platform integrate with Epic?"
A behavioral health provider asks: "Do you support Cerner?"
Your first enterprise customer says: "We're using Meditech. How quickly can your system connect with our environment?"
Suddenly, EHR integration for mental health platforms stops being a future roadmap item. It becomes a growth requirement.
This is where many teams discover that mental health platform EHR integration development is far more complicated than moving patient records between systems or connecting APIs.
Questions like these start appearing quickly:
Many teams start by asking whether newer standards automatically mean better integrations.
That is usually the wrong place to start.
The real challenge is understanding what your developers should actually build when healthcare organizations rarely operate using a single interoperability standard.
Whether you're investing in FHIR R4 EHR integration mental health platforms, building HL7 v2 EHR integration mental health software, expanding telehealth capabilities, or creating intelligent behavioral health products through AI mental health app development initiatives, integration decisions made early can determine whether your platform scales smoothly or creates expensive technical debt later.
Many teams jump straight into the FHIR versus HL7 debate.
In reality, choosing standards before understanding integration requirements is often where expensive mistakes begin.
Before deciding what your developers should build, it's important to understand why EHR integration for mental health platforms has become a business necessity rather than a technical enhancement.
If you're building a mental health platform today, here's a question worth asking:
Can your product function effectively if clinicians still need to manually switch between multiple systems every day?
For most organizations, the answer is no.
EHR integration for mental health platforms refers to the process of enabling your platform to securely exchange data with Electronic Health Record systems used by healthcare providers, hospitals, behavioral health organizations, and clinical networks.
The objective is straightforward.
Your platform should fit into existing clinical workflows instead of forcing providers to create new ones.
For most companies, mental health platform EHR integration development typically includes connecting systems that handle:
Whether you're planning a complete behavioral health ecosystem or a telehealth EHR integration mental health platform build, interoperability becomes the layer that allows all these workflows to work together.
A few years ago, integration was often treated as a competitive advantage.
Today, buyers increasingly treat it as a requirement.
Healthcare organizations expect new software investments to work alongside the infrastructure they already use.
That shift creates several realities for mental health companies:
This is why many teams discover that building features are rarely the hardest part.
Building features that integrate with real healthcare environments usually is.
Many founders also search for this question early in the process:
What is the difference between FHIR R4 and HL7 v2 EHR integration for mental health platforms and when should developers use each standard?
The answer depends on your customers, the EHR systems they use, and the workflows your platform needs to support.
Before deciding what your developers should build, it's important to understand how these standards work and why choosing incorrectly can create expensive integration problems later.
Healthcare interoperability is booming, with the market expected to surpass $9 billion soon. Missing this now could cost you later.
Talk to Integration ExpertsMost teams approaching EHR integration for mental health platforms start with the same question:
Should we build using FHIR R4 or HL7 v2?
The problem is that many teams treat this as a technology comparison when it's really an architecture decision.
FHIR R4 and HL7 v2 solve different problems, operate differently, and often coexist within the same healthcare environment.
If you're evaluating FHIR R4 EHR integration mental health platforms initiatives or planning HL7 v2 EHR integration mental health software, here's what your development team needs to understand first:
|
Factor |
FHIR R4 |
HL7 v2 |
|---|---|---|
|
Core Purpose |
Built to support modern, API-driven interoperability between EHRs, third-party applications, telehealth products, mobile apps, and patient-facing systems. |
Built to exchange healthcare events and operational data between clinical systems using structured messages. |
|
Communication Model |
Request-response architecture where applications retrieve or update data through API calls when required. |
Event-driven architecture where systems automatically send messages when clinical events occur. |
|
Data Format |
Uses JSON or XML formats that align with modern development practices and cloud architectures. |
Uses pipe-delimited messages that require specialized parsing and healthcare integration expertise. |
|
Developer Experience |
Easier for modern engineering teams because it closely resembles conventional API development patterns. |
Requires deeper understanding of healthcare message structures, interface design, and integration workflows. |
|
Learning Curve |
Lower learning curve for teams experienced with APIs, web services, and SaaS platforms. |
Higher learning curve due to message mapping, segment structures, triggers, acknowledgements, and interface management. |
|
Authentication & Security |
Supports OAuth 2.0, SMART on FHIR, OpenID Connect, granular scopes, refresh tokens, and modern access controls. |
Authentication often depends on interface engines, VPNs, network controls, or custom security implementations. |
|
Real-Time Data Access |
Supports on-demand retrieval of patient records, appointments, assessments, observations, and clinical resources. |
Primarily distributes updates when specific healthcare events generate messages. |
|
Behavioral Health Data Support |
Better suited for structured handling of assessments such as PHQ-9, GAD-7, patient questionnaires, observations, and care plans. |
Often requires custom mappings and extensions to support behavioral health workflows consistently. |
|
Therapy & Psychiatric Workflows |
Commonly used for patient engagement tools, teletherapy platforms, behavioral health apps, and care coordination systems. |
Frequently supports scheduling updates, admissions, referrals, discharge notifications, and operational workflows. |
|
SMART App Integration |
Supports embedded SMART applications directly inside EHR workflows. |
Does not provide native support for embedded applications. |
|
Epic Integration Support |
Strong API ecosystem through App Orchard, SMART on FHIR frameworks, and modern interoperability programs. |
Continues supporting many operational workflows through HL7 interfaces. |
|
Cerner Integration Support |
Extensive API support through Oracle Health interoperability initiatives and FHIR ecosystems. |
Commonly encountered in existing enterprise implementations with established interface infrastructure. |
|
Meditech Integration Support |
Support varies depending on deployment environment, interoperability modules, and platform versions. |
Still commonly encountered for operational messaging and legacy workflow integrations. |
|
Data Granularity |
Applications can request only the specific resources, fields, or encounters required. |
Systems typically exchange entire message payloads even when only small portions are needed. |
|
Scalability |
Easier scaling using API gateways, cloud services, microservices, and distributed infrastructure. |
Operational complexity increases as interfaces, message volumes, and integrations expand. |
|
Error Handling & Debugging |
Standardized API responses make troubleshooting, logging, and monitoring easier for engineering teams. |
Errors often require message tracing, interface monitoring, and deeper investigation. |
|
Infrastructure Requirements |
Usually built using APIs, middleware, authorization servers, cloud services, and modern integration layers. |
Often requires interface engines, message brokers, transformation layers, and dedicated integration infrastructure. |
|
Implementation Timeline |
Typically faster for greenfield healthcare products and modern technology stacks. |
Usually longer due to mapping complexity, testing cycles, interface configuration, and validation requirements. |
|
Development Cost & Maintenance |
Lower long-term maintenance because API architectures are generally easier to extend and maintain. |
Higher operational overhead due to interface monitoring, maintenance, and custom message handling. |
|
Best Mental Health Use Cases |
Telehealth platforms, behavioral health applications, patient portals, therapy platforms, analytics systems, and AI-powered healthcare products. |
ADT feeds, hospital event notifications, referral workflows, scheduling updates, and legacy healthcare integrations. |
|
What Developers Commonly Get Wrong |
Teams often assume every vendor exposes identical FHIR resources, scopes, and workflows, which frequently causes delays during testing and certification. |
Teams frequently underestimate message mapping complexity, interface maintenance effort, and operational overhead. |
|
Mental Health Platform Recommendation |
Usually the preferred starting point for patient-facing experiences, modern behavioral health workflows, and scalable platform development. |
Often remains necessary when connecting with hospitals and health systems still operating large HL7-based ecosystems. |
|
Long-Term Industry Direction |
Continues expanding through interoperability mandates, API adoption, and healthcare modernization initiatives. |
Remains critical because many healthcare organizations continue relying heavily on existing HL7 infrastructure. |
Looking at the table, many founders immediately ask: Does this mean FHIR R4 replaces HL7 v2?
Not really.
The reality is that most healthcare organizations operate in mixed environments where both standards exist simultaneously.
This is exactly why many teams building mental health software EHR integration technical guide roadmaps discover that choosing one standard exclusively often creates problems later.
Understanding how these standards differ technically is where the real architecture decisions begin.
Many teams building FHIR R4 EHR integration mental health platforms start with a simple assumption:
FHIR is newer, so we should build with FHIR.
That assumption is only partially correct. FHIR R4 has become one of the most important interoperability standards in healthcare, but understanding why it matters is more important than simply adopting it.
Let's start with the basics.
FHIR stands for Fast Healthcare Interoperability Resources. It is a healthcare interoperability standard developed to make data exchange between healthcare systems easier, faster, and more developer-friendly.
Unlike older healthcare integration approaches that depend heavily on message feeds and custom interfaces, FHIR R4 uses modern API principles that many engineering teams already understand.
This means your developers can work with:
Think of FHIR R4 as a standardized API layer that allows healthcare applications to securely access and exchange clinical information without building completely custom integrations every time.
This is one reason why mental health EHR integration FHIR R4 development continues growing across behavioral health platforms.
A common misconception is that FHIR simply "moves patient records." It does much more than that.
When teams develop FHIR mental health app EHR integration, they typically use FHIR to support workflows such as:
Imagine a therapist opening your platform and instantly viewing patient history, medications, recent assessments, and appointment details without switching between multiple systems.
That's the kind of workflow FHIR is designed to support.
Healthcare organizations are increasingly adopting modern interoperability strategies. As a result, FHIR R4 EHR integration mental health platforms have become attractive because FHIR works well with how modern software is built.
Some reasons teams prefer FHIR include:
API-based architectures are generally easier for engineering teams to build, maintain, and scale compared to traditional message-based integrations.
FHIR works particularly well for:
One major advantage is SMART on FHIR mental health platform integration. SMART on FHIR allows applications to launch directly inside EHR environments while maintaining secure authentication and patient context. This becomes especially valuable when building clinician-facing experiences or Epic SMART on FHIR mental health app integration workflows.
Many organizations investing in healthcare AI increasingly rely on interoperable data pipelines. Teams building products around AI driven EHR MVP development or expanding AI automation services initiatives often discover that structured APIs simplify downstream automation significantly.
Not every healthcare workflow benefits equally from FHIR. Here is where FHIR typically performs best:
|
Mental Health Use Case |
FHIR R4 Fit |
Why It Works |
|---|---|---|
|
Teletherapy platforms |
Excellent |
Supports patient-facing workflows, scheduling, and clinical data access |
|
Behavioral health assessments |
Excellent |
Works well with questionnaires, observations, and structured outcomes |
|
Patient portals |
Excellent |
Designed for secure patient access and mobile experiences |
|
Care coordination platforms |
Excellent |
Simplifies information sharing across providers |
|
AI-powered behavioral health solutions |
Excellent |
Structured APIs simplify data ingestion and automation |
|
Remote monitoring solutions |
Excellent |
Supports ongoing patient data exchange |
|
Hospital event notifications |
Moderate |
Often requires additional systems or HL7 support |
|
Legacy hospital workflows |
Limited |
Many environments still depend on older interoperability standards |
This is where many teams get surprised. FHIR is powerful. FHIR is not universal.
Healthcare organizations rarely operate identical environments.
Some common limitations include:
This is why many organizations discover that FHIR R4 EHR integration mental health platforms projects rarely remain purely FHIR-based forever.
Many integration problems are not caused by poor engineering. They're caused by incorrect assumptions.
Some mistakes appear repeatedly:
Teams investing in AI integration services, connected care platforms, or broader healthcare ecosystems often discover that successful integrations depend more on architecture decisions than technology selection.
And this brings us to the next question. If FHIR solves many modern interoperability problems, why does HL7 v2 still remain deeply embedded across healthcare systems?
Modern APIs are only part of the challenge. Real complexity lies in workflows, auth, and vendor compatibility.
Discuss Your FHIR StrategyAfter learning about FHIR R4, many founders and CTOs ask the same question: If FHIR is the modern standard, why are healthcare organizations still using HL7 v2?
The answer is simple.
Because healthcare doesn't replace infrastructure overnight. Many hospitals, health systems, behavioral health organizations, laboratories, pharmacies, and payer networks have spent decades building workflows around HL7 v2. Replacing those systems is often expensive, disruptive, and unnecessary when existing integrations continue to perform reliably.
This is why HL7 v2 EHR integration mental health software remains a critical part of healthcare interoperability, even in organizations actively adopting FHIR.
HL7 v2 is a messaging standard developed by Health Level Seven International (HL7) for exchanging healthcare information between systems. Unlike FHIR, which typically uses APIs to request data when needed, HL7 v2 works by sending messages automatically when specific events occur.
Think of it this way:
For example:
Each event can trigger an HL7 message that is sent to connected systems. This event-driven approach is one reason HL7 remains deeply embedded across healthcare environments.
Many teams assume HL7 only handles patient demographics. In reality, HL7 often supports some of the most important operational workflows within healthcare organizations.
When organizations implement mental health platform EHR integration development, HL7 v2 frequently handles:
For behavioral health organizations, these events help ensure care teams receive timely information without manually checking multiple systems.
A therapist may not need to query an API every few minutes to see whether a patient has been admitted to a facility. Instead, the appropriate HL7 message can notify connected systems automatically.
This is where many technology teams underestimate healthcare complexity. Most healthcare organizations operate large ecosystems made up of:
Many of these systems were built long before FHIR existed. As a result, HL7 continues supporting thousands of operational workflows that healthcare organizations rely on every day.
Common reasons organizations continue using HL7 include:
Many HL7 interfaces have been operating successfully for years.
Healthcare organizations are often reluctant to replace systems that already work well.
HL7 excels at distributing notifications when something changes. For many hospital workflows, this remains more efficient than continuously requesting information through APIs.
Most large healthcare organizations already maintain:
Replacing that infrastructure can require significant investment.
HL7 continues to perform exceptionally well in specific scenarios.
|
Mental Health Use Case |
HL7 v2 Fit |
Why It Works |
|---|---|---|
|
Patient admissions and discharges |
Excellent |
Event-driven architecture immediately distributes updates |
|
Appointment scheduling updates |
Excellent |
Changes can be automatically shared across systems |
|
Referral management |
Excellent |
Supports provider-to-provider communication workflows |
|
Hospital event notifications |
Excellent |
Designed specifically for event-driven healthcare communication |
|
Registration and insurance updates |
Excellent |
Widely supported across healthcare systems |
|
Care coordination notifications |
Excellent |
Ensures relevant teams receive timely updates |
|
Patient-facing mobile applications |
Limited |
Not designed for modern app experiences |
|
Teletherapy platforms |
Limited |
FHIR generally provides a better developer experience |
|
Embedded EHR applications |
Poor |
Does not support SMART-style app experiences |
|
AI-driven behavioral health platforms |
Moderate |
Useful for event notifications but often requires FHIR for deeper data access |
While HL7 remains important, it also introduces challenges for modern development teams.
Some of the most common limitations include:
For engineering teams accustomed to APIs and cloud-native architectures, HL7 can initially feel unfamiliar.
This is one reason many organizations now combine HL7 and FHIR rather than relying exclusively on either standard.
We've seen teams make the same mistakes repeatedly.
Even though organizations use the same standard, implementations often vary. Custom segments, workflows, and message requirements are common.
Building the interface is only part of the effort. Monitoring, troubleshooting, message validation, and ongoing support often require significant operational attention.
HL7 is older than FHIR. That doesn't mean it's obsolete. Many mission-critical healthcare workflows still depend on HL7-based infrastructure.
One of the most expensive mistakes occurs when teams assume they must choose between FHIR and HL7. In reality, many successful healthcare products use both. This is especially true when supporting Epic, Cerner, Meditech, and other healthcare ecosystems simultaneously.
And that raises an important question: What happens when your platform needs FHIR for modern APIs and HL7 for legacy healthcare workflows at the same time?
That's where hybrid integration architecture becomes essential.
If your mental health platform only needs to connect with a single EHR environment, choosing between FHIR R4 and HL7 v2 may seem straightforward.
However, most healthcare organizations don't operate in a single-standard environment. A hospital may expose FHIR APIs for patient-facing applications while continuing to rely on HL7 v2 for admissions, scheduling updates, referrals, and operational workflows.
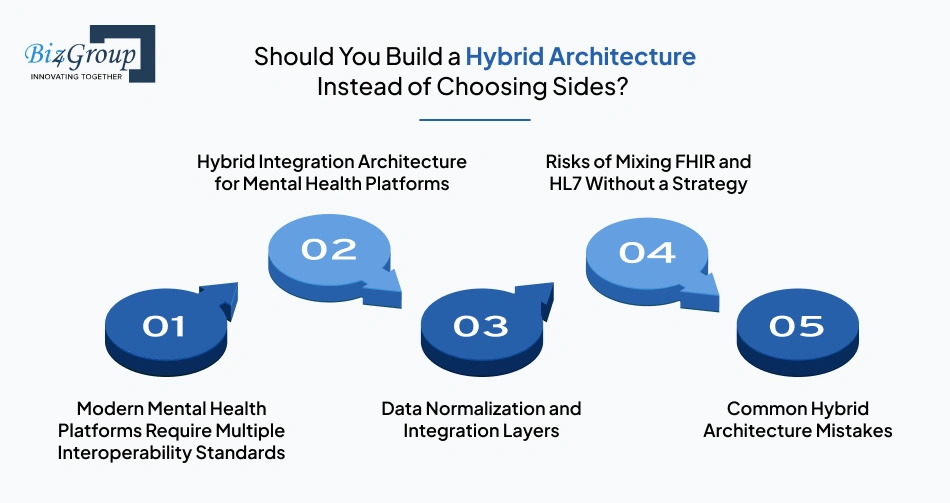
This is why many successful EHR integration for mental health platforms projects are built around hybrid architectures rather than choosing one standard over the other.
Healthcare ecosystems are rarely uniform. A mental health platform serving multiple providers may encounter Epic, Cerner, Meditech, and other systems, each with different interoperability capabilities and requirements. As a result, teams often discover that how to build a mental health platform EHR integration architecture that supports both FHIR R4 and HL7 v2 standards for connecting with different EHR systems simultaneously becomes a more relevant question than choosing a single standard.
A hybrid architecture allows your platform to leverage FHIR where modern APIs provide value while continuing to support HL7 workflows that healthcare organizations still depend on. For example, your application might retrieve patient records, assessments, and medication history through FHIR while receiving admissions, referrals, and scheduling updates through HL7 messages. This approach creates flexibility without limiting future integration opportunities.
One of the biggest challenges in mental health platform EHR integration development is handling data coming from multiple sources and standards. A normalization layer helps transform FHIR resources, HL7 messages, and vendor-specific formats into a consistent internal data model. This makes application logic simpler, improves reporting accuracy, and reduces downstream development complexity.
Organizations building intelligent healthcare products often follow similar principles when implementing AI integration services, where multiple systems and data formats must work together seamlessly.
Using both standards does not automatically create a better architecture. Problems usually appear when teams connect systems directly without defining ownership, transformation rules, synchronization logic, or data governance policies. This is one reason when should mental health platform developers use FHIR R4 versus HL7 v2 integration standards and why mixing them carelessly causes critical integration failures remains a common concern among health IT leaders.
The most expensive integration problems often originate from architectural decisions made early in development.
Common mistakes include:
The strongest architectures are designed around business workflows first and interoperability standards second.
That foundation becomes especially important once you begin connecting with Epic, Cerner, Meditech, and other enterprise healthcare environments at scale.
Whether you're looking to build EHR integration mental health telehealth platform capabilities or support enterprise behavioral health workflows, successful integrations require much more than connecting APIs and exchanging data.
The strongest implementations are built around interoperability standards, clinical workflows, security requirements, and long-term scalability.
Here's what your development team should focus on.
Many integration projects run into delays because teams start building before fully understanding the systems they need to connect. One of the first challenges is determining how to decide between FHIR R4 and HL7 v2 EHR integration for a mental health platform connecting to Epic Cerner and Meditech simultaneously. The answer depends on customer requirements, EHR capabilities, and workflow complexity.
Key activities include:
Secure access is one of the most important components of mental health platform EHR integration development. Modern healthcare applications increasingly rely on SMART on FHIR mental health platform integration frameworks to manage authentication, authorization, and patient context securely. This becomes especially important during Epic SMART on FHIR mental health app integration projects where access scopes and permissions are tightly controlled.
Your team should plan for:
Different EHR vendors often represent similar information in different formats. Teams looking to create mental health app EHR integration FHIR workflows quickly discover that data normalization becomes essential for maintaining consistency across multiple systems. Without it, every new integration introduces additional complexity.
Important considerations include:
As integration requirements grow, direct system-to-system connections become difficult to maintain. A middleware layer acts as the central hub for routing, validating, transforming, and monitoring data exchanged across systems. This becomes particularly valuable when organizations need to integrate AI with EHR/EMR systems while supporting traditional interoperability workflows.
Core components often include:
An integration isn't production-ready simply because data is flowing successfully. Every HL7 FHIR mental health platform developer guide should emphasize testing because vendor sandboxes rarely mirror production environments perfectly. Thorough validation helps prevent delays during certification and go-live phases.
Testing should include:
EHR integrations require ongoing operational oversight long after deployment. Any effective mental health software EHR integration technical guide should treat monitoring as a core operational function rather than an afterthought. Systems evolve, APIs change, and healthcare workflows continue to expand over time.
Production readiness should include:
By this stage, your team should have a clear understanding of what a production-ready integration architecture looks like. The next challenge is often more strategic than technical: deciding which EHR vendors to prioritize, how much integration effort to budget for, and what factors should influence your roadmap before development begins.
Authentication, data mapping, and middleware are just the start. Planning right saves months of rework.
Plan Your Integration Roadmap
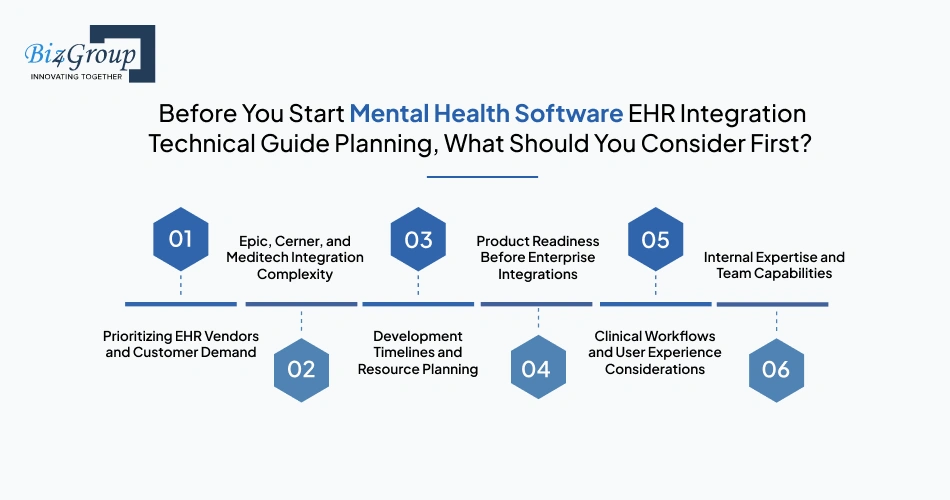
Building integrations before understanding business priorities often creates expensive technical debt later. Before committing engineering resources, it's important to evaluate where integrations create the most value, what your customers actually need, and how much operational complexity your team can realistically support.
Many teams assume they need Epic, Cerner, and Meditech integrations immediately. In reality, prioritization should depend on customer demand, target market, sales pipeline, and implementation complexity. Enterprise customers often influence integration priorities more than technical preferences. Understanding where your users operate should guide roadmap decisions before development begins.
Not all EHR integrations require the same effort. Epic API integration mental health platform development projects may provide modern APIs and SMART workflows, while Cerner EHR integration mental health app development often introduces different operational requirements. Meditech EHR integration mental health platform projects can become significantly more complicated depending on deployment environments and interoperability capabilities.
One of the biggest mistakes teams make is underestimating implementation effort. Building telehealth EHR integration mental health platform build capabilities often requires significantly more engineering effort than expected because integration work extends beyond development into testing, validation, security reviews, certification, and operational monitoring. Teams should budget time for both technical work and vendor-related delays.
Many startups attempt enterprise integrations before validating whether customers actually need every planned capability. Organizations pursuing MVP development strategies often discover that focusing on high-value workflows first creates faster feedback loops and reduces unnecessary integration complexity. Starting smaller frequently leads to better architectural decisions later.
Technical integration alone does not guarantee adoption. Poor workflows, excessive clicks, fragmented experiences, and inconsistent data presentation can create frustration even when integrations work correctly. Strong UI/UX design decisions become especially important when clinicians interact with multiple systems throughout the day.
Healthcare interoperability requires specialized knowledge that many engineering teams encounter for the first time during implementation. Teams often underestimate the complexity involved in interoperability standards, vendor certification processes, security requirements, and operational support. This is why many organizations evaluate whether to build expertise internally, partner externally, or expand teams before large-scale integration efforts begin.
These considerations may feel less technical than FHIR resources or HL7 messages, but they often determine whether integration projects stay on schedule, stay within budget, and successfully reach production environments.
Many teams build mental health platform EHR integration development without fully understanding the pitfalls. This table summarizes the most common failure points, their causes, and how to prevent them.
|
Failure Point |
Why It Happens |
How to Avoid |
|---|---|---|
|
Unrealistic Integration Assumptions |
Teams assume all EHR vendors expose identical APIs, FHIR resources, or HL7 message structures. |
Conduct detailed discovery with each EHR vendor; validate sandbox behavior against production; adjust architecture to account for differences. |
|
Poor Architecture Decisions |
Early designs choose a single standard or lack hybrid capabilities, creating scalability and maintenance issues. |
Build hybrid architecture plans that can support both FHIR R4 and HL7 v2; define ownership of data flows and transformation rules. |
|
Underestimating Vendor Complexity |
Teams assume Epic, Cerner, and Meditech integrations are interchangeable. |
Prioritize vendor integrations based on customer demand and technical complexity; allocate realistic timelines and resources. |
|
Security and Compliance Oversights |
Teams fail to account for HIPAA, OAuth scopes, SMART on FHIR authorization, or audit requirements. |
Implement robust authentication, role-based access, logging, and access monitoring; review compliance with security experts. |
|
Operational and Scaling Challenges |
Integrations work initially but fail at scale due to data volume, message frequency, or API rate limits. |
Design integration layers with monitoring, retry logic, and error handling; simulate expected load before production deployment. |
|
Building Without Specialized Healthcare Expertise |
Developers unfamiliar with FHIR, HL7, EHR vendor nuances, or behavioral health workflows make critical mistakes. |
Engage experienced health IT developers or consultants; leverage hire mental health platform developers in USA when needed. |
The reality is that most integration failures are rarely caused by a single technology decision.
They usually happen because teams underestimate complexity, prioritize speed over architecture, or treat interoperability as a feature instead of a core platform capability.
The good news?
Most of these mistakes are preventable when your team understands what production-ready healthcare integrations actually require.
And that raises another important question:
Who should you trust to build something this complex when EHR integration mistakes can impact timelines, budgets, enterprise deals, and long-term scalability?
Building EHR integration for mental health platforms requires more than connecting APIs or exchanging healthcare messages.
Teams must account for interoperability standards, authentication workflows, behavioral health data structures, vendor-specific requirements, certification processes, and production-scale architecture.
At Biz4Group, we work with healthcare organizations building platforms that require reliable interoperability across modern APIs, legacy healthcare systems, and enterprise clinical workflows.
Whether the requirement involves Epic API integration mental health platform development, Cerner EHR integration mental health app development, or Meditech EHR integration mental health platform environments, the focus remains the same: building architectures that can support production healthcare workloads rather than isolated integrations.
Our teams support organizations building connected healthcare ecosystems through AI healthcare software development company expertise, scalable enterprise AI solutions, and advanced agentic AI development capabilities.
Because successful interoperability is rarely determined by a single integration decision.
It is usually determined by whether the underlying architecture can continue supporting new vendors, new workflows, and growing enterprise requirements without expensive rework.
Correct architecture early means scaling across Epic, Cerner, Meditech, FHIR, and HL7 is smoother.
Talk With Biz4GroupBuilding EHR integration for mental health platforms requires much more than connecting systems. Successful implementations depend on interoperability expertise, scalable architecture, security planning, and understanding how real healthcare environments operate.
At Biz4Group, we help organizations build interoperable healthcare solutions that support modern APIs, legacy systems, behavioral health workflows, and enterprise-scale requirements across complex healthcare ecosystems.
Because building integrations is one thing.
Building integrations that continue working as your platform grows is something else.
If building healthcare interoperability feels complicated, you're probably building something worth doing. Let's build it correctly.
EHR integration for mental health platforms means securely exchanging clinical and operational data between your application and Electronic Health Record systems used by hospitals and provider networks. It's essential because enterprise customers expect connected clinical workflows instead of isolated systems, and without integration your platform can struggle to deliver complete patient data or close enterprise contracts.
FHIR R4 and HL7 v2 are two interoperability standards used to connect systems with EHRs. FHIR R4 is a modern RESTful API‑based standard designed for real‑time access to clinical data, while HL7 v2 EHR integration mental health software relies on event‑driven message feeds for workflows like admissions and scheduling. Both often coexist because many hospitals support HL7 v2 for legacy workflows even as FHIR adoption accelerates.
Choosing between FHIR R4 EHR integration mental health platforms and HL7 v2 depends on your product needs and customer environment. FHIR R4 is typically best for APIs, patient‑facing apps, and modern workflows, while HL7 v2 remains necessary for real‑time event feeds like ADT notifications and legacy system integrations. In many cases a hybrid approach gives the broadest compatibility.
Yes. Major EHR vendors such as Epic and Cerner support FHIR R4 APIs for modern interoperability, with Epic offering FHIR via its App Orchard and Cerner providing FHIR endpoints through its developer portal. However, many organizations still require HL7 v2 EHR integration mental health software for operational interfaces alongside FHIR APIs.
Production‑ready EHR integration timelines vary but are generally longer than basic API development. Beyond coding, teams must plan for sandbox connectivity, vendor documentation review, security approvals, testing, and certification, which can extend projects into months rather than weeks. Realistic estimates depend on targeted EHR vendors and the complexity of workflows being integrated.
Teams often underestimate differences in FHIR resource availability across EHR systems and treat sandbox behavior as production behavior. Another common mistake is assuming SMART authorization flows will handle all context automatically without addressing workflow differences across vendors. Planning for these nuances up front improves success rates.
Yes. mental health platform EHR integration development can support a wide range of clinical data including structured assessments, encounter records, medication histories, and progress notes. Modern standards like FHIR R4 are particularly suited for structured resources, but teams often need custom mapping and data normalization when integrating legacy HL7 v2 workflows or vendor‑specific extensions.

with Biz4Group today!
Our website require some cookies to function properly. Read our privacy policy to know more.