info@biz4group.com
info@biz4group.com 






























Imagine a digital system that doesn’t wait for instructions but instead, understands your business goals, learns from real-time feedback, and takes independent actions to get the job done.
Read More

What happens to your mental health platform the day a patient's therapy notes, crisis records, and diagnosis history end up somewhere they should not?
Not hypothetical. A question every founder and CTO in this space needs to answer before it becomes their reality.
PHI data architecture for mental health platforms is not a compliance checkbox you revisit before launch. It is the structural foundation that determines whether your platform survives a breach or becomes another case file in an OCR enforcement action. And when you are dealing with mental health platform PHI security architecture, the margin for error is razor thin.
The stakes in behavioral health are higher than most healthcare categories. According to the IBM Cost of a Data Breach Report 2025, the average healthcare data breach now costs $9.77 million, the highest of any industry for the fourteenth year running. Mental health platforms are increasingly targeted precisely because the data they hold is sensitive, and the architectural gaps are predictable.
At Biz4Group, we have designed and built HIPAA-compliant AI healthcare software across telehealth platforms, multi-provider therapy networks, and behavioral health startups at various stages of growth. One thing we see consistently: teams do not get breached because they ignored security. They get breached because they treated compliance as a documentation exercise rather than an engineering discipline.
A signed BAA, encryption at rest, some access logging, and a policy PDF. That combination gets presented as a compliance posture more often than it should. It is not a HIPAA-compliant database design for mental health apps. It is a structure that holds up fine during normal operations and falls apart the moment it is actually tested.
Here is what that looks like in practice: a mid-stage mental health startup reaches Series B, a security review gets triggered by an enterprise client, and the team discovers their audit trail cannot tell them which provider accessed which patient records or when. Not because no one logged anything, but because the logging schema was never designed with breach scoping in mind. That is a fixable problem, but it is expensive and disruptive to fix under pressure.
The decisions that protect your platform happen at the database level. Which fields get field-level PHI encryption for healthcare apps treatment and which do not. How multi-provider access control for mental health platforms is structured across care roles. Whether your audit trail implementation in healthcare apps can scope a breach in hours rather than weeks. Whether your cloud HIPAA-eligible services for mental health apps configuration are genuinely compliant or just adjacent to it.
Getting secure PHI storage for mental health platforms right from the start is not just about avoiding fines. It is about building something that enterprise clients trust, that survives investor due diligence, and that holds up when a real incident puts your systems under pressure.
If you are working through questions like "we are building a mental health platform and want to design PHI data architecture that is fully HIPAA-compliant with encryption, RBAC, and audit trails", this is written directly for you.
Let's get into it.
Over 275 million healthcare records have been breached since 2009. Most of those platforms thought they were compliant too.
Let's Audit Your ArchitectureMost HIPAA data protection strategies for mental health apps get designed as if behavioral health data is just another category of healthcare records. It is not. The regulatory obligations are different, the data sensitivity is higher, and the architectural decisions that follow from that are more complex than a standard healthcare app requires.
If you are building in this space and treating PHI the same way a billing platform or a general EHR would, you are already working with an incomplete picture.
HIPAA governs all PHI, but mental health platforms often carry a second federal obligation, which applies to substance use disorder records and requires explicit patient consent even for treatment-related disclosures.
On top of that, psychotherapy carries restrictions that standard clinical notes do not. They cannot be disclosed without separate patient authorization, cannot be used for payment or operations purposes, and must be stored separately from the rest of the medical record.
If your schema does not account for both of these layers from day one, you are not building HIPAA-compliant database design for mental health apps. You are building something that will require expensive restructuring the moment a compliance review or enterprise client asks the right questions.
The 18 HIPAA identifiers are the baseline, but on a mental health platform the PHI surface area is wider than most teams expect.
Session notes, diagnosis codes, crisis intervention records, medication history, mood tracking data, and even appointment scheduling metadata all qualify. Here is the one that catches teams off guard: an appointment confirmation message that references your practice name can constitute a PHI disclosure if your practice name reveals the nature of the treatment.
When you are designing best practices in mental health app design, mapping every data touchpoint against the full PHI definition is not optional. It is the foundation everything else is built on.
Not all PHI on a mental health platform carries the same regulatory weight, and your schema should reflect that distinction directly.
Here is the classification framework we apply when designing mental health platform PHI security architecture:
Tier 1: Standard PHI: Name, date of birth, contact details, insurance information. Standard HIPAA protections apply.
Tier 2: Clinical Mental Health Records: Diagnosis codes, treatment plans, session notes, and medication history. Requires field-level encryption and role-scoped access.
Tier 3: Psychotherapy Notes: Therapist process notes maintained separately from the medical record. Requires separate schema, separate encryption keys, and separate authorization workflow.
Tier 4: 42 CFR Part 2 SUD Records: Substance use disorder treatment records. Requires data segmentation, explicit consent verification before any disclosure, and exclusion from routine TPO pipelines.
Each tier maps to a different set of encryption requirements, access control rules, and audit logging obligations. Building this classification into your schema from the start is what separates a platform built for secure PHI storage for mental health platforms from one that just looks compliant on the surface.
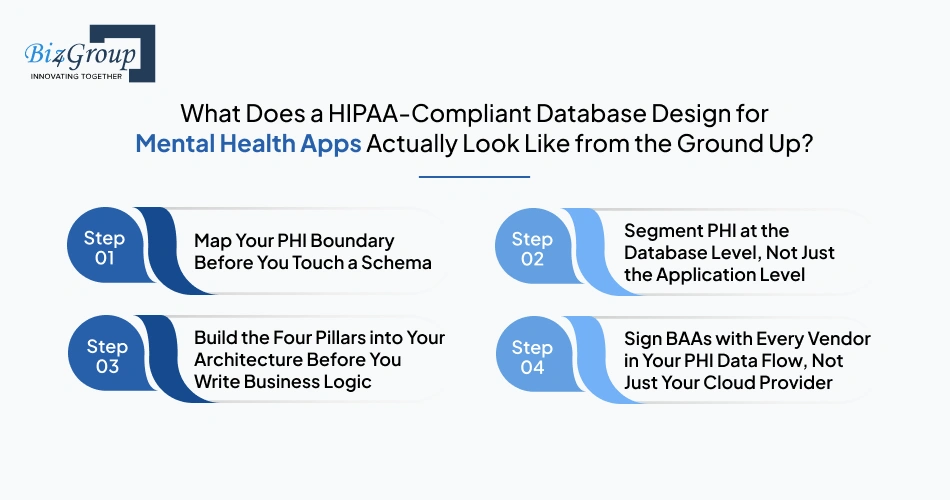
Most teams start with the schema and retrofit compliance later. That is the wrong order. HIPAA-compliant database design for mental health apps starts with understanding what you are protecting, where it lives, and who can touch it before a single table gets created.
Here is the sequence we follow when building PHI data architecture for mental health platforms from scratch.
Your PHI boundary defines every system, service, and data flow that touches protected health information. Without it, you cannot scope your encryption requirements, your BAA obligations, or your audit trail coverage accurately.
Application-layer separation is not enough. A bug, a misconfigured role, or a compromised service account can bypass application controls entirely. Secure PHI storage for mental health platforms requires isolation in the database layer itself.
This is where most platforms cut corners under time pressure. The four pillars of mental health platform PHI security architecture need to be in place before any feature development touches patient data, not added on top of it afterward.
Building healthcare software product development workflows around these four pillars from the start is what keeps a platform from needing a full architectural overhaul six months before a major enterprise deal closes.
Teams sign a BAA with AWS or Azure and assume the obligation is covered. It is not. Every vendor that touches PHI, including your logging provider, your analytics tool, your email delivery service, and any AI model your platform calls, needs a signed BAA before any patient data flows through it.
These four steps are not a one-time setup exercise. They are the ongoing operational posture that keeps your HIPAA data protection strategies for mental health apps functional as your platform scales, adds providers, and brings on new integrations. If you are asking "we are a digital health company planning our database for multi-provider mental health apps and need guidance on PHI field-level encryption and access control", the answer always starts here, with boundary mapping and structural segmentation, before anything else gets built on top.
Knowing the framework is one thing. Having a team that has done it before is another.
Talk to Our PHI Architecture TeamA signed BAA and basic encryption get you to the starting line. What happens between the starting line and an actual breach is determined by three specific controls that most mental health platforms either implement partially or skip entirely.
There are three controls that consistently separate platforms that survive security incidents from ones that do not. If your engineering team cannot clearly explain how each of these is implemented in your system, that is the conversation you need to have before anything else.
Think of encryption in layers. The outermost layer protects your entire database if someone physically compromises your server. That is full-disk encryption, and yes, you need it. But it does nothing if someone gets in through a compromised user account or an over-privileged access role, which is the far more common scenario.
Field-level PHI encryption for healthcare apps adds protection inside the database itself. Individual fields like therapy notes, diagnosis codes, and medication history are encrypted at the column level. Even if someone gets into your database, those fields are unreadable without the right decryption key.
The practical question to ask your team: which specific fields in our database are encrypted at the column level, and which are relying only on disk-level protection?
Key things to have in place:
How to secure mental health app databases with field-level PHI encryption is one of the most searched questions among digital health CTOs, and the answer always comes back to this: disk encryption is the floor, not the ceiling.
RBAC, role-based access control, means people only access the data their role actually requires. On a single-provider platform that is manageable. On a multi-provider mental health platform serving group practices, telehealth networks, or care coordination programs, it gets complicated fast.
A primary therapist should only see their own caseload. A supervising clinician may need to read access across supervised providers. A billing user needs claim data but not clinical notes. An on-call provider needs temporary emergency access without permanent broad permissions.
When these distinctions are not built into your access architecture, you end up with over-permissioned roles that expose more data than necessary. That is not a hypothetical risk. It is one of the most common findings in healthcare security audits.
Here is a simplified version of the access matrix we recommend for HIPAA-compliant PHI storage and access control for multi-provider mental health systems:
|
Role |
Patient Records |
Clinical Notes |
Billing Data |
|---|---|---|---|
|
Patient |
Own only |
Own only |
Own only |
|
Primary Therapist |
Own caseload |
Full access |
None |
|
Supervising Clinician |
Supervised caseload |
Read only |
None |
|
Care Coordinator |
Program-scoped |
Treatment plan only |
None |
|
Billing Staff |
De-identified only |
None |
Full access |
|
Platform Admin |
None |
None |
None |
|
On-Call Provider |
Temporary, time-limited |
Time-limited |
None |
The question to ask your team: does our access control model reflect this level of role specificity, and is it enforced at the database layer or only at the application layer?
Application-layer access control alone is not enough. A code bug or misconfigured API can bypass it. Access rules need to be enforced at the database level so that even if something breaks above it, the data stays protected.
Your audit trail is your single most important asset when something goes wrong. It answers the questions that determine your regulatory exposure: who accessed what, when, and which patients were affected.
Most platforms log something. The problem is that what gets logged is usually not enough to answer those questions with any precision. And under HIPAA's 60-day breach notification requirement, imprecise answers create serious liability.
Audit trail implementation in healthcare apps for mental health platforms needs to capture:
The field most teams leave out is the one that matters most during a breach: which specific PHI categories were accessed. Without it, you cannot scope your notification obligation accurately. You end up either over-notifying, which damages patient trust, or under-notifying, which creates regulatory exposure.
Beyond what you log, how you store it matters just as much. Audit logs need to be:
If your audit trail can be altered after the fact, it is not a compliance asset. It is a liability.
The three controls above work as a system. Field-level PHI encryption for healthcare apps limits what an attacker can read. RBAC design for HIPAA-compliant mental health platforms limits who can get there. And audit trail schema design and immutability requirements for HIPAA mental health apps tells you exactly what happened when something goes wrong despite the other layers being in place.
If you are asking "we are designing a mental health platform and want to implement audit logging and immutability for HIPAA compliance", these three controls together are the answer. And as AI in mental health becomes a core part of more platforms, every AI feature that touches patient data needs to operate within this same control framework, not outside it.
Choosing a cloud provider for your mental health platform is not just an infrastructure decision. It is a compliance decision. All three major providers, AWS, Azure, and GCP, offer HIPAA-eligible services and will sign a BAA. But signing a BAA does not make your deployment compliant. Your configuration does.
The differences between the three providers matter depending on what your platform needs to do, how it is built, and where it is headed. Here is how they compare across the criteria that matter most for cloud PHI storage using AWS, GCP, or Azure for healthcare apps:
|
Criteria |
AWS |
Azure |
GCP |
|---|---|---|---|
|
HIPAA-Eligible Services |
150+ services, deepest catalog in healthcare |
Strong catalog, tighter Microsoft ecosystem integration |
Solid catalog, strongest for AI and analytics workloads |
|
Key Management |
AWS KMS, supports customer-managed keys and automatic rotation |
Azure Key Vault, HSM-backed, integrates tightly with Azure AD |
Cloud KMS, customer-managed encryption keys (CMEK) across all PHI storage |
|
Audit Logging |
CloudTrail + CloudWatch, comprehensive but requires configuration |
Azure Monitor + Microsoft Defender for Cloud, strong threat detection |
Cloud Audit Logs + Security Command Center, clean and straightforward |
|
Identity and Access Control |
AWS IAM, powerful but requires significant expertise to configure correctly |
Azure Active Directory, strongest for enterprise and Microsoft-stack teams |
Identity-Aware Proxy, zero-trust access model, simpler syntax than AWS IAM |
|
Network Isolation |
VPC with private subnets, security groups, no public IP on PHI databases |
Virtual Network with private endpoints, strong enterprise network controls |
VPC Service Controls, prevents data exfiltration even from within the cloud environment |
|
Mental Health Specific Services |
Amazon HealthLake for FHIR-native clinical data storage and querying |
Azure API for FHIR, strong for interoperability requirements |
Cloud Healthcare API, supports FHIR, HL7v2, strong for data pipelines |
|
Best Fit For |
Platforms that need the widest HIPAA-eligible service catalog and healthcare-specific tooling |
Teams already in the Microsoft ecosystem or building for enterprise health systems |
Platforms with strong AI, analytics, or interoperability requirements |
|
Notable Certifications |
SOC 1/2/3, ISO 27001, FedRAMP, HITRUST CSF |
SOC 1/2/3, ISO 27001, FedRAMP, HITRUST CSF |
SOC 1/2/3, ISO 27001, FedRAMP |
One thing all three have in common: none of them are compliant by default. Encryption, access control, audit logging, and network segmentation all need to be configured explicitly. The most common and costly cloud HIPAA-eligible services for mental health apps mistakes we see are not provider selection errors. They are configuration errors that would have happened on any platform.
The three that appear most often:
If you are asking "we are evaluating cloud HIPAA-eligible services like AWS, GCP, and Azure for storing PHI in our mental health platform", the right answer is not which provider is most compliant. It is which provider your team can configure and maintain correctly given your stack, your scale, and your roadmap.
The top mental health app features that drive engagement and retention, things like real-time messaging, AI-assisted assessments, and crisis detection, all generate PHI that flows through this cloud infrastructure. Getting the foundation right is what makes those features safe to build and scale.
Most development teams can build a mental health app. Fewer can build one where the PHI data architecture for mental health platforms is designed correctly from day one, where the encryption, access control, and audit trail decisions are made with compliance in mind rather than bolted on afterward.
At Biz4Group, we have spent 20 years building healthcare and mental health products for founders and CTOs who needed a technical partner that understood both the product and the compliance landscape. We do not hand you a generic HIPAA checklist and call it architecture. We design systems where HIPAA-compliant database design for mental health apps is a structural decision, not an afterthought.
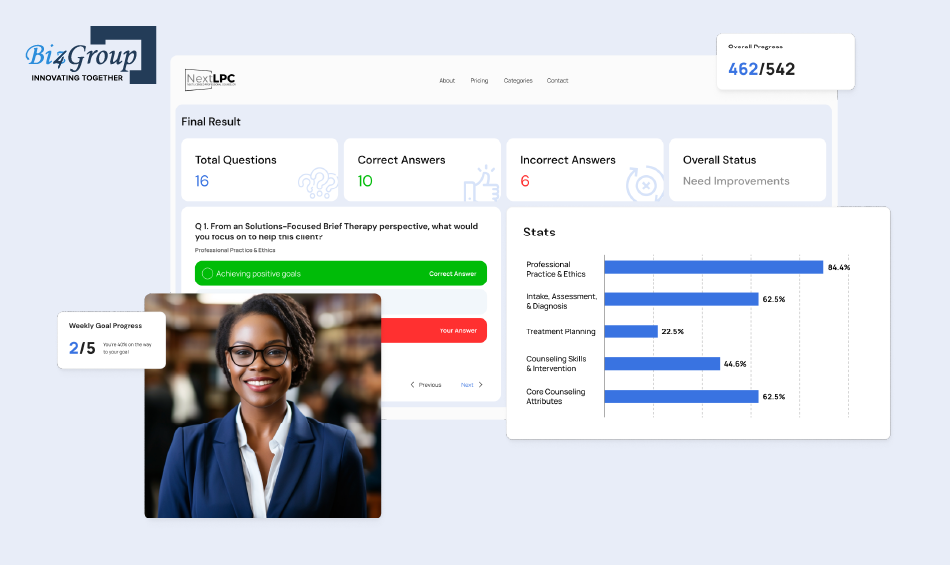
One project that reflects this directly is NextLPC, an AI-powered platform we built for psychotherapy students where AI avatars act as therapy tutors, guiding students through real case studies and assessments. Building in the therapy and mental health space meant handling sensitive educational and clinical content with care, designing access controls that matched the platform's specific user roles, and building a system the client trusted completely.
Here is what Dr. Tiffinee Yancey, CEO of NextLPC, said about working with us:
"Biz4Group's AI development team has been outstanding. Their excellent communication, timely delivery, innovative solutions, and genuine commitment to our project have made a significant impact."

We also built AI Wizard, an AI-powered companion platform offering empathy-driven voice and video interactions, which required thoughtful handling of emotionally sensitive user data and careful design around user privacy and data boundaries.
If you are asking "we are looking for a company that can design PHI data architecture for HIPAA-compliant mental health platforms" or "we want end-to-end PHI data architecture services for mental health apps with HIPAA compliance, encryption, and breach handling", that is exactly the kind of work we do.
You can hire mental health app developers in USA from our team who have hands-on experience building in this space or reach out directly to discuss your platform's specific architecture requirements.
We have built this space. We know exactly where the gaps appear and how to close them.
Let's Build It the Right WayPHI data architecture for mental health platforms is not a problem you solve once and move on from. It is an ongoing engineering discipline that determines how your platform handles growth, audits, enterprise sales, and the inevitable moment when your security posture gets tested.
The decisions covered in this guide, from your PHI boundary and data classification framework to field-level PHI encryption for healthcare apps, multi-provider RBAC design, immutable audit trails, and cloud configuration, are not theoretical. They are the difference between a breach that your platform recovers from and one that defines it permanently.
Mental health data carries a weight that most other healthcare data does not. The patients on your platform trusted you with some of the most sensitive information in their lives. Getting the architecture right is not just a regulatory obligation. It is the foundation of trust.
At Biz4Group, we have built across the mental health and healthcare space long enough to know where the gaps appear, what they cost, and how to close them before they become a problem. Our team brings the technical depth and domain experience to design HIPAA-compliant database design for mental health apps that holds up under real scrutiny, not just on paper.
If you are ready to build a mental health platform that is secure, compliant, and built to scale, connect with our team and let us get to work.
PHI data architecture for mental health platforms is the structural design of your databases, encryption layers, access controls, and audit systems built specifically to protect patient health information in a behavioral health context. Mental health platforms carry a heavier regulatory burden than most healthcare apps, psychotherapy notes, substance use disorder records, and even scheduling metadata all fall under stricter disclosure rules. A generic healthcare architecture does not account for any of that.
No. Signing a BAA defines the shared responsibility model. It does not configure your encryption, enable your audit logging, or segment your PHI databases. Cloud HIPAA-eligible services for mental health apps are compliant platforms. Your deployment on top of them may or may not be, depending entirely on how it is configured. The BAA is the starting point, not the finish line.
Yes, you need both. Full-disk encryption protects against physical theft. Field-level PHI encryption for healthcare apps protects against the far more common scenario: a compromised account or misconfigured access role that exposes patient data through the application layer. For mental health platforms, psychotherapy notes and substance use disorder records should use entirely separate encryption keys from the rest of your data.
Map your full role taxonomy before writing any access control code. Designing RBAC access matrices for multi-provider mental health platforms means defining exactly what each role needs to see and nothing beyond that. Once the matrix is defined, enforce it in the database layer through row-level security, not just the application layer. Application controls can be bypassed. Database layer enforcement cannot.
Your audit trail implementation in healthcare apps needs to capture user ID, role at time of access, patient record involved, action taken, reason for access, IP address, outcome, and which specific PHI fields were exposed. That last field is what allows you to scope a breach precisely. Logs must be stored in an append-only, tamper-proof system separate from your application database and retained for a minimum of six years.
It means encryption and MFA are effectively mandatory now, even before the rule is finalized. HIPAA-compliant database design for mental health apps built to the proposed standard today avoids expensive retrofits later. The proposed rule also introduces a 24-hour breach notification obligation for business associates and requires annual penetration testing. Building these standards now is significantly cheaper than fixing gaps under a compliance deadline.
Directly. Without a properly designed audit trail and access controls that limit breach of blast radius, scoping an incident can take weeks. Breach notification and compliance for PHI systems depends on knowing which patients were affected, which records were accessed, and whether data was encrypted at the time. Teams with the right architecture scope a breach in hours. Teams without it risk missing the deadline or over-notifying their entire patient population.

with Biz4Group today!
Our website require some cookies to function properly. Read our privacy policy to know more.