info@biz4group.com
info@biz4group.com 






























Imagine a digital system that doesn’t wait for instructions but instead, understands your business goals, learns from real-time feedback, and takes independent actions to get the job done.
Read More
You built the feature. The mood check-ins work. The AI is reading patterns. The UI looks clinical enough to close any enterprise deal.
Then your legal advisor asks one question: "Is this thing a medical device?"
The room goes quiet.
If you are building AI mood tracking in mental health apps in 2026, that moment is not hypothetical. It is happening to product teams every single week, and the ones caught off guard are paying for it in stalled launches, rejected App Store submissions, and compliance fires they never budgeted for.
Here is why this keeps catching teams by surprise.
The space is growing faster than most regulatory understanding of it. According to a report, the global mental health app market was valued at $8.9 billion in 2025 and is projected to reach $17.52 billion by 2030, growing at a CAGR of 14.6 percent. At the same time, another report found that 23 percent of U.S. adults experienced a mental illness in the past year, with the majority receiving no treatment at all. That treatment gap is exactly what is driving CTO after CTO to prioritize AI-powered mood analytics in mental health apps right now.
But market opportunity and regulatory complexity are moving at the same speed. And most development teams are tracking only one of them.
The FDA updated its digital health guidance in January 2026, redrawing lines that your product roadmap probably has not accounted for yet. The FTC ordered BetterHelp to pay $7.8 million and Cerebral to pay over $7 million for mishandling mental health data, and neither case had anything to do with FDA clearance. Enterprise buyers are running full compliance reviews before signing any digital mental health vendor. App stores are flagging submissions that lack proper clinical disclaimers.
So, the real question is not whether AI mood tracking in mental health apps is worth building. It clearly is. The question is whether you know exactly which side of the FDA line your feature sits on right now.
Most teams who set out to build an AI mental health app do not have a clear answer to that. Not because they are careless, but because the classification rules are genuinely complex, they shifted again in 2026, and almost nothing written for builders explains them in plain language.
At Biz4Group, with 20 plus years of software development experience and a dedicated track record in healthcare AI, we have worked with mental health platform teams navigating exactly this crossroads. We know what the right architecture looks like before the first line of code gets written, and we know what it costs when teams skip that step.
This guide covers FDA regulations for AI mood tracking in apps including the SaMD versus general wellness distinction, what the 2026 updates actually change for your product, how to implement PHQ-9 and GAD-7 safely, and what it takes to build digital health AI mood tracking solutions that hold up under regulatory, enterprise, and clinical scrutiny.
No recycled compliance checklists. No content written for lawyers. Just a straight answer on where the lines are drawn and what you need to do about it.
One of the most common questions we get from founders early in the scoping process goes something like this: "We want to add mood tracking to our mental health app. How complicated can it really be?"
Pretty complicated. And the teams that figure that out after they have already shipped are the ones calling lawyers.
So, before we get into regulation and compliance, let us get clear on what AI mood tracking in mental health apps actually means in a product context, because the term is being used to describe everything from a basic emoji check-in to a sophisticated behavioral pattern engine. That gap matters enormously, both for what you build and for how regulators look at it.
A simple mood log where a user picks how they feel today? That is mood tracking.
An AI that reads a user's journal entry, detects linguistic patterns linked to low affect, cross-references that against a 14-day trend, and adjusts what therapeutic content gets served next? That is also mood tracking.
But these are not the same product. They do not carry the same regulatory risk. They do not require the same development decisions. And if your team is treating them as equivalent during the planning phase, that is where the problems start.
Depending on your product architecture, it can include any combination of the following:
Each of these sits at a different point on the regulatory spectrum. Some are clearly general wellness. Some push you toward FDA oversight depending entirely on how you build them and, more importantly, how you describe them. That distinction is what this entire guide is built around.
We have seen this shift happen in real time across the healthcare AI projects we have worked on. Three things converged and changed the conversation completely.
Enterprise buyers stopped giving the benefit of the doubt. Health systems, insurers, and employee assistance programs evaluating AI mental wellness monitoring tools are now asking about regulatory classification, clinical validation, and data handling in the first sales call. Not the third. Not during legal review. The first call. Teams that cannot answer those questions clearly do not make it a follow-up conversation.
Reimbursement pathways that did not exist two years ago are now open. CMS established new codes for digital health AI mood tracking solutions, and the FDA launched the TEMPO pilot in January 2026 to bring digital health devices to Medicare and Medicaid patients. The products positioned to capture that reimbursement are the ones that were built with clinical architecture from day one, not bolted on later when a contract required it.
Clinical credibility became the actual competitive moat. The AI mental health applications for monitoring mood and emotional wellness that are winning enterprise deals are the ones with validated instruments, documented outcomes, and a clear answer to the compliance question. Pure consumer wellness apps, no matter how well designed, cannot compete on that ground.
And then there is the question that keeps coming up from product leads who are further along in the build: "We are designing AI mood tracking features in our mental health app and we want to know the clinical validation requirements and risk implications. Where does our specific feature land?"
The honest answer is it depends on decisions your team is making right now, possibly without realizing their regulatory weight.
The FDA does not regulate your technology. It regulates your intent. Two apps can run the exact same underlying AI model for mood tracking AI for mental health platforms and land in completely different regulatory categories based on nothing more than the language used to describe what the app does. In your app store listing. In your onboarding copy. In your investor deck.
That is the thing most development guides skip entirely. And it is exactly what we are going to walk through in detail.
In our experience building AI-driven health platforms where sensitive data, real-time monitoring, and compliance decisions intersect, the teams that get this right share one thing in common. They made the classification decision before writing a single line of code, not after their first enterprise prospect asked them to prove it.
That is the position we want to help you build from.
The mental health app market hits $9.45 billion in 2026 and only 14 percent of platforms report clinically validated outcomes.
Let's Talk About Your AppHere is a question we hear from product leads who are already mid-build: "We are a mental health startup and we want to understand FDA regulations for AI mood tracking in apps. But everything we read feels outdated. What actually changed in 2026?"
Quite a lot. And if your team has not reviewed the regulatory updates from this year, you are building on an incomplete picture. Here are the four changes that matter most for your product right now.
On January 6, 2026, FDA Commissioner Martin Makary announced two updated guidance documents at the Consumer Electronics Show in Las Vegas. His framing was direct: "We have a clear lane for medical-grade products, but otherwise, we need to adapt with the times and be proactive with guidance so that companies and developers are not left confused about what they should be doing or what the FDA wants."
The two documents he was referring to:
General Wellness: Policy for Low Risk Devices — superseding the 2019 version, this update gives mental health app builders something genuinely useful. Products can now prompt users to consult a healthcare professional when outputs fall outside normal thresholds and still qualify as general wellness, provided the notification does not name a specific disease, does not categorize outputs as abnormal or diagnostic, and does not include any clinical recommendations.
For a mood tracking app, "your check-ins have looked different lately, consider speaking with someone" is wellness language. "Your PHQ-9 score indicates moderate depression" is not.
The guidance also explicitly lists "a claim that a product helps treat an anxiety disorder" as a disqualifying example. If that language exists anywhere in your app store listing, onboarding screens, or marketing copy, you are in regulated territory regardless of what your technology actually does.
Clinical Decision Support Software — the operative version is dated January 29, 2026. The most relevant change for AI mood tracking features that feed into clinical workflows: single-output CDS can now qualify for enforcement discretion, but only when no other clinically appropriate option exists and the clinician remains firmly in the decision-making loop. This is a meaningful shift from the 2022 version but it is not a broad deregulation of AI clinical tools.
One update that went largely unnoticed: the FDA also withdrew its guidance on SaMD Clinical Evaluation on the same day. Teams following that international framework for their validation strategy need to reassess.
In November 2025, the FDA's Digital Health Advisory Committee convened its second-ever meeting, focused entirely on generative AI in digital mental health medical devices.
Two things came out of that meeting that every CTO in this space needs to know.
First, as Psychiatric Times reported in its direct coverage of the session, the FDA has authorized over 1,200 AI-enabled medical devices to date but has not authorized a single AI device for any mental health purpose. Not one therapy chatbot. Not one diagnostic mood tool. Not one LLM-based mental wellness product. And as STAT News confirmed in March 2026, no generative AI device has received full FDA authorization for any clinical indication at all. If you are building a conversational AI mood companion and assuming that regulatory path has been cleared by someone else, it has not.
Second, the DHAC flagged a specific technical requirement that most development teams are not aware of. Any AI mood assessment in mental health applications that learns from user data and adapts its behavior over time likely needs a Predetermined Change Control Plan, or PCCP, filed before deployment. Without one, every meaningful algorithm update could require a brand new regulatory submission. This is the FDA's stated position from its August 2025 PCCP guidance, reinforced at the November meeting.
The FDA's Quality Management System Regulation became effective February 2, 2026. It replaces the old Quality System Regulation and incorporates ISO 13485:2016 by reference, aligning U.S. quality requirements with the international standard used by regulators across the EU, Canada, Australia, and Japan.
If your app crosses into SaMD territory, your quality system documentation must now map to ISO 13485 structure. Risk management must be embedded across your entire quality system, not treated as a standalone document. The old inspection framework is gone as of February 2, 2026.
If you started QMS documentation before that date, audit it against the new standard before you get anywhere near a 510(k) submission.
The FDA launched the TEMPO pilot in January 2026, in partnership with CMS's ACCESS model. Behavioral health, covering depression and anxiety, is one of the four confirmed clinical use areas in the Federal Register. The FDA plans to select up to 10 U.S.-based manufacturers in the behavioral health category.
The practical opportunity: manufacturers can request FDA enforcement discretion for certain requirements while deploying their device under the ACCESS model and collecting real-world evidence in parallel. It is a structured pathway to get a behavioral health AI tool in front of Medicare and Medicaid patients and build toward full FDA authorization without needing a completed clinical trial as the entry requirement.
One important clarification worth stating plainly: TEMPO is not a shortcut around device regulation. Participants collect real-world performance data under active FDA oversight and are expected to work toward a future marketing submission.
The first cohort application window closed April 1, 2026. The next entry point is January 1, 2027. If you are at the MVP development stage for your AI mental health app and thinking about how to build a credible path toward reimbursement, TEMPO is the most significant new option available right now.
The 2026 regulatory picture is not simply more lenient or more strict. It is more precise. The FDA drew sharper lines between genuinely low-risk wellness tools and AI-powered clinical mental health features. The teams that benefit are the ones who made their classification decision deliberately and built their architecture to match it.
The question is not whether these updates affect your product. They do. The question is which side of them you are on.
Your compliance strategy is already behind if your team has not reviewed the January 2026 guidance update.
Get a Compliance ReviewMost founders building AI mood tracking in mental health apps spend all their compliance energy on the FDA question. That makes sense. But the FDA is not the only regulator paying attention to this space, and some of the most expensive mistakes teams make have nothing to do with medical device classification at all.
Here is what else you need to have a handle on.
HIPAA compliance applies when your app qualifies as a covered entity or business associate handling Protected Health Information. The trigger most teams miss: the moment your mood tracking data connects to a licensed provider, flows into an EHR, or gets processed by a third-party analytics tool, a Business Associate Agreement is required. Every vendor that touches PHI needs a signed BAA before a single byte of patient data moves through their system. No BAA means a potential violation even if your own security is airtight. The best practices in mental health app design make HIPAA architecture a day-one decision, not a retrofit.
This is the compliance framework that caught BetterHelp and Cerebral off guard. The FTC's updated Health Breach Notification Rule, effective July 2024, explicitly covers health and wellness apps that are not subject to HIPAA. If your mood tracking app collects mental health data and shares it with any third party without explicit user authorization, including advertising platforms or analytics tools, that can constitute a breach under the rule. General wellness classification from the FDA does not exempt you from FTC enforcement. These are two entirely separate regulatory tracks.
If your mental health platform handles any substance use disorder records alongside mood tracking data, 42 CFR Part 2 applies on top of HIPAA. Enforcement for the updated Part 2 rules began February 16, 2026. The practical implication: SUD records carry stricter consent and disclosure restrictions than standard PHI. A BAA is not sufficient for handling SUD data. You need a Qualified Service Organization Agreement instead. Many behavioral health platforms building mood tracking features are touching SUD data without realizing it.
Eight additional state comprehensive privacy laws came into effect in 2025, several of which treat mental health data as a sensitive category requiring explicit opt-in consent rather than the standard opt-out model. If your app has users in California, Washington, Nevada, or Texas, you are operating under state-level mental health data protections that go beyond federal requirements. This is not theoretical exposure. State attorneys general are actively enforcing these laws, and mental health data is consistently flagged as a high-priority category.
Both Apple and Google require mental health apps to include crisis resource access and clinical disclaimers when the app addresses anxiety, depression, mood, or emotional wellness. Apple specifically requires that any app discussing suicide or self-harm provide access to crisis support resources. These are not suggestions. Non-compliant submissions get rejected, and apps already live in the store can be pulled. Your mental health app mood tracking compliance strategy needs to account for app store requirements as a separate workstream from FDA and FTC obligations.
Getting all five of these right simultaneously is genuinely complex. They do not always point in the same direction, and a decision that satisfies one framework can create exposure under another. That is exactly why hiring mental health app developers in the USA who understand the full compliance stack matters more in this space than in almost any other category of app development.
This is the question every founder building in this space eventually has to answer. And most of them answer it too late. After the architecture is set, after the app store copy is written, the first enterprise prospect asks for a compliance summary.
So let us work through it properly.
SaMD stands for Software as a Medical Device. The FDA defines it as software intended to perform a medical purpose, such as diagnosing, treating, monitoring, or predicting a health condition, without being part of a hardware device.
General Wellness is software that promotes a healthy lifestyle or general state of health without making claims related to diagnosing, curing, treating, or preventing a specific disease or condition.
The key word in both definitions is intended. It is not about what your software technically does. It is about what you say it does, in your app, in your marketing, and in your documentation.
Here is how the two categories compare across the dimensions that matter most for mood tracking AI for mental health platforms:
Dimension |
General Wellness |
SaMD |
|---|---|---|
Intended use |
Promote healthy habits, emotional reflection, stress management |
Diagnose, treat, monitor, or predict a specific mental health condition |
Mood tracking claims |
"Track how you feel and reflect on patterns" |
"Screen for depression" or "monitor bipolar symptoms" |
PHQ-9 / GAD-7 use |
Self-reflection tool, clearly framed as not diagnostic |
Scores used to generate clinical recommendations or flag a diagnosis |
AI output |
Informational insights the user acts on independently |
Outputs that influence or replace a clinical decision |
Provider integration |
No clinical workflow connection |
Shares data with licensed providers or integrates with EHR systems |
Notification language |
"Your check-ins look different lately, consider speaking with someone" |
"Your score indicates moderate depression" |
Marketing copy |
"A wellness companion for your emotional health" |
"Clinically validated tool for detecting depressive episodes" |
FDA oversight |
Enforcement discretion applies, no clearance required |
Premarket clearance required (510(k), De Novo, or PMA) |
Documentation needed |
Written wellness classification rationale |
Full QMS, clinical validation, algorithm documentation, cybersecurity controls |
The single factor that decides everything is how broadly the FDA reads intended use. It is not just your in-app copy. It is your App Store listing, your marketing website, your press releases, your investor pitch deck, and your support documentation. Your public communications establish your intended use whether you realize it or not.
Before you finalize any AI mood assessment in mental health applications feature, run it through these:
If you answered yes to any of these, a Pre-Submission meeting with the FDA before you finalize your architecture is the right next step. If you answered no to all five, document that rationale in writing and keep it updated as your product evolves.
The smarter approach for most teams is to build a mental health app like BetterHelp or similar platforms with regulatory scalability in mind from day one. Design your wellness features to stay clearly in wellness territory, document your classification rationale, and architect in a way that allows you to upgrade toward SaMD without rebuilding from scratch if your product roadmap eventually requires it.
One wrong classification decision can cost you an enterprise contract, an App Store listing, or both.
Talk to Our Team Today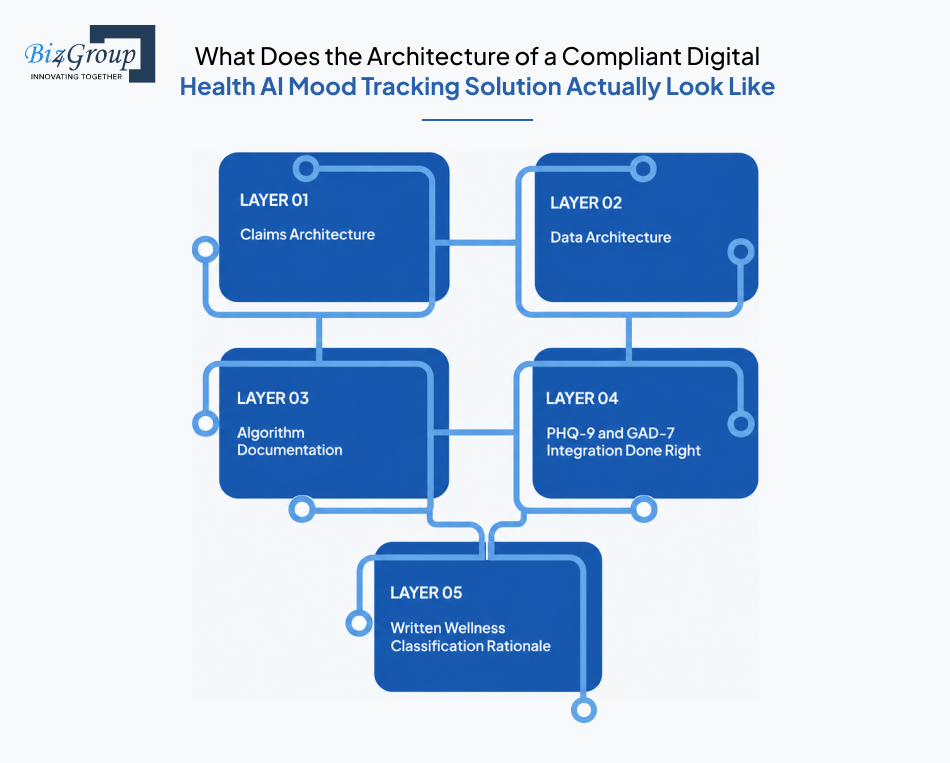
Most teams think about compliance after the product is built. That is exactly when it costs the most to fix. The teams building digital health AI mood tracking solutions that survive enterprise due diligence, App Store reviews, and regulatory scrutiny all have one thing in common: they made these architectural decisions before sprint one, not after launch.
If you are asking "we are designing AI mood tracking features in our mental health app and want to know clinical validation requirements and risk implications" - this section answers that question layer by layer.
Here are the five layers that make the difference.
Every word your product says to users, investors, app stores, and the press is establishing your intended use in the FDA's eyes. Before a single screen gets designed, every team building a mental health app mood tracking compliance strategy needs a claims audit. This means reviewing all user-facing copy against the wellness vs. SaMD line we covered in the previous section. The UI/UX design layer is not just a visual exercise in digital health. It is a regulatory document.
How you collect, store, and move mood tracking data determines your HIPAA exposure, your FTC risk, and in some cases your AI mood tracking in mental health apps with FDA compliance considerations. Getting this wrong at the architecture stage means rebuilding your data layer under pressure. The right time to decide what counts as PHI, where it lives, who can access it, and what third-party tools touch it is before you choose your stack.
If your AI-based mood tracking and clinical assessment in mental health apps ever needs to demonstrate regulatory defensibility, to the FDA, to an enterprise buyer, or in a product liability context, your algorithm documentation is the evidence. Most teams either do not have it or create it retrospectively, which carries far less weight than documentation built in parallel with development.
These are the two instruments developers ask about most and get wrong most often. Teams building AI mental health applications for monitoring mood and emotional wellness consistently underestimate the regulatory weight of these instruments. Using PHQ-9 and GAD-7 in your app does not automatically make it SaMD. How you implement them and what you do with the scores is what determines your regulatory position.
If your team is asking: "we want to integrate AI mood assessment with PHQ-9 and GAD-7 in our mental health platform and understand compliance obligations" — these bullet points are your starting checklist:
This is the document most teams never create, and it is the one that protects you most when things get serious. Teams ask: "We want to avoid regulatory penalties and need to understand clinical validation and documentation requirements for AI mood tracking in mental health apps." This document is your first line of defense. A written wellness classification rationale is a one-to-two-page internal document that explains, with reference to the FDA's 2026 General Wellness guidance, exactly why your product qualifies for enforcement discretion rather than device regulation.
Building all five layers correctly from the start is exactly what separates the AI mental wellness monitoring tools closing enterprise contracts from the ones stuck in compliance remediation. If you want to see what a mental wellness app like Headspace gets right architecturally, the answer almost always traces back to decisions made before the first line of code was written.
One of the most common questions product teams ask us sounds like this: "We are exploring AI mental health tools and want to understand recent FDA enforcement actions affecting mood tracking apps. Which of our specific features actually trigger regulation?"
The honest answer is that regulation is not triggered by your product category. It is triggered by specific feature decisions. Two apps in the same category can sit on opposite sides of the line based entirely on what individual features claim to do.
The FDA itself uses a three-tier risk framework for digital mental health software: Not a Device, Enforcement Discretion, and Focus of Regulatory Oversight. Every feature your app ships falls into one of those three buckets.
Here is the straight breakdown by feature type. No gray zone language. Just where each one sits and why.
Feature |
Regulatory Status |
Why |
|---|---|---|
Daily mood journal with emoji or scale logging |
✅ Not a Device |
No clinical claims. User reflects on emotional state. No AI interpretation generating recommendations. Confirmed in FDA's own DHAC presentation. |
Sentiment analysis on free-text journal entries |
✅ Not a Device |
AI reads emotional tone and surfaces patterns for user awareness. Informational only, no clinical output. |
PHQ-9 or GAD-7 administered as self-reflection check-in |
✅ Enforcement Discretion (with correct framing) |
Instrument used for reflection, not screening. Score displayed without clinical interpretation. Framing is everything. |
Mood trend visualization over time |
✅ Not a Device |
Showing a user their own data pattern is informational, not diagnostic. |
Push notification: "Your check-ins look different lately" |
✅ Not a Device |
No disease reference, no diagnostic label, no clinical threshold. Meets the 2026 four-condition test. |
App providing "Skill of the Day" coping technique to anxious users |
✅ Enforcement Discretion |
Directly confirmed by FDA's DHAC presentation as a low-risk example where FDA intends to exercise enforcement discretion. |
AI that interprets PHQ-9 scores and recommends treatment |
🔴 Focus of Regulatory Oversight |
Score interpretation generating a clinical recommendation crosses the line immediately. |
Mood-based escalation alert sent to a clinician |
🔴 Focus of Regulatory Oversight |
Output influences a clinical decision. Clinician-facing workflow is a strong SaMD signal. |
AI that adjusts therapeutic content based on clinical mood scores |
⚠️ Gray Zone |
Depends entirely on claims. Wellness framing may be defensible. Treatment adjustment framing is SaMD. |
Generative AI conversational companion with mood monitoring |
🔴 Focus of Regulatory Oversight |
No GenAI mental health device has been authorized by the FDA as of 2026. The November 2025 DHAC meeting addressed this category directly. Do not launch without regulatory counsel. |
PHQ-9 data shared with a licensed provider via provider dashboard |
🔴 SaMD plus HIPAA triggered |
Clinical workflow integration plus PHI sharing. Both SaMD classification and BAA requirement apply. |
Passive behavioral signal detection (session frequency, login time) |
✅ Not a Device |
Collecting behavioral metadata for wellness insights without clinical claims stays in wellness territory. |
Crisis escalation routing when PHQ-9 Item 9 is endorsed |
✅ Required Safety Feature |
Routing to crisis resources is a safety obligation, not a clinical claim. Must be built regardless of classification. |
The ⚠️ gray zone row deserves a direct explanation because it is where most teams get into trouble.
Adaptive content delivery driven by mood patterns is not automatically SaMD. The FDA confirmed at the November 2025 DHAC meeting that it would exercise enforcement discretion for an app helping patients with anxiety by providing a daily skill, even when it technically meets the definition of a medical device. What pushes an adaptive feature into regulated territory is the claims language around it, not the underlying mechanism.
The technology can be identical. The regulatory outcome is entirely different.
For teams asking "we are struggling to integrate mood tracking algorithms safely and need guidance on compliance and risk management" - the answer in almost every case comes back to claims architecture, not algorithm architecture. Fix the language first. Document the wellness rationale. Then build.
If your feature landed in the red column, you have three options:
Knowing where your feature sits is step one. Building it right is where most teams need help.
Start Building the Right WayGetting your regulatory classification right is one thing. Having a development team that can actually build to it is another. This is the gap most founders discover too late, usually when an enterprise buyer asks a technical compliance question their dev team cannot answer.
Here is what to look for, and what to walk away from.
Most software development firms are genuinely good at building software. What they are not equipped for is the intersection of AI, HIPAA architecture, FDA regulatory strategy, and clinical validation simultaneously. These are four distinct disciplines that rarely exist under one roof, and in digital mental health, you need all four from day one. A team that treats HIPAA as a checkbox and has never heard of a Pre-Submission Q-Sub meeting is not the right partner for building clinically validated AI mood tracker features, regardless of how impressive their portfolio looks.
When you are evaluating a development partner for AI mental health app clinical validation work, these signals should end the conversation early:
Any one of these alone is a problem. More than one and you are looking at a team that will hand you a liability, not a product.
The right partner for building AI mood tracking in mental health apps with FDA compliance considerations does not just write clean code. They understand the regulatory weight of every product decision and help you make them correctly from the start.
These questions will tell you everything you need to know about whether a development partner actually understands this space or is learning on your budget:
A partner who cannot answer these questions clearly and confidently is telling you something important. The right AI app development company for this space has thought through all of these scenarios before your first scoping call, not during it.
This is not just a compliance argument. It is a business argument. Enterprise health systems, insurers, and employee assistance programs are all asking these exact questions during vendor evaluation now. If your development partner built your app without answers to them, your sales cycle stalls at the first compliance review. A team that understands AI mental health app clinical validation requirements from the start means your product enters enterprise conversations with documentation, not apologies. That difference directly affects your time to revenue, your fundraising story, and your defensibility in due diligence. The teams who treat compliance as an architectural input rather than an afterthought are the ones closing the contracts everyone else is losing.
You can hire AI developers who understand code. The harder thing to find is a team that understands code and the regulatory, clinical, and commercial environment it is being deployed into.
Because most development firms make you choose between moving fast and building right. We do not.
At Biz4Group, with 20 plus years of software development experience, 300 plus dedicated professionals, and 1,000 plus successful projects delivered, we have built across healthcare AI, wellness platforms, and conversational AI long enough to know where the expensive mistakes happen. In AI mood tracking in mental health apps, they almost always happen before the first line of code gets written.
Here is what our work actually looks like.
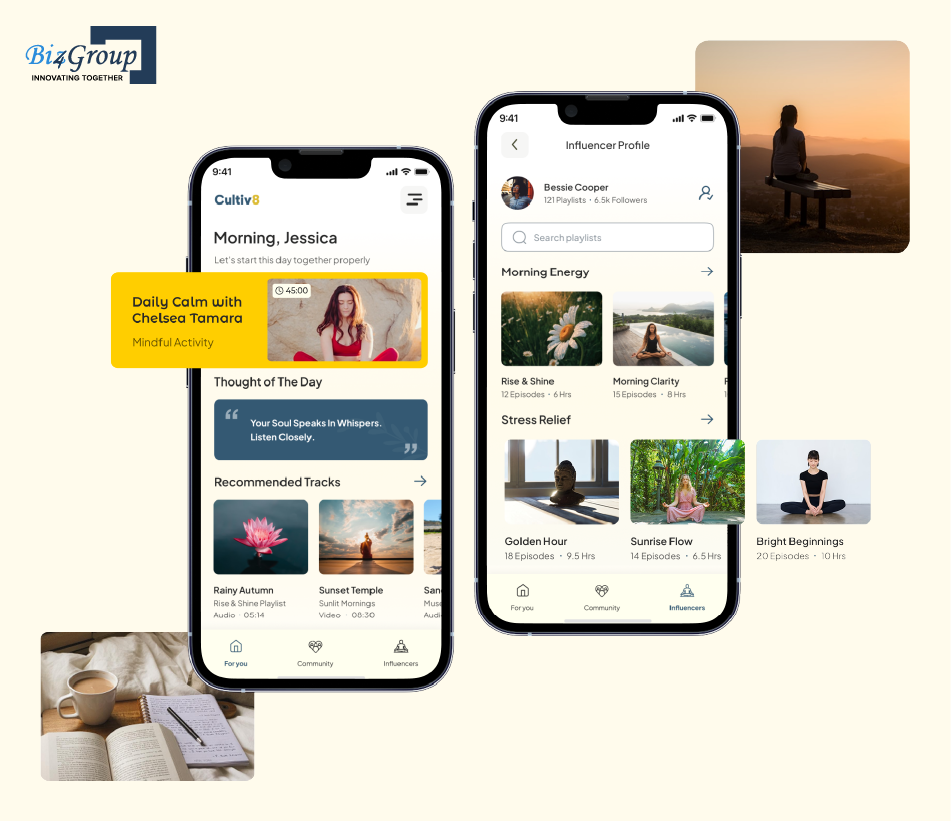
Cultiv8 is a meditation and spiritual wellness platform we built from the ground up. The platform handles personalized practice recommendations, community features, and sensitive user wellness data at scale across a growing user base.
What made this build relevant to digital health AI mood tracking solutions was not just the wellness context. It was the data architecture decisions we made throughout. User privacy, data minimization, and delivering genuinely personalized experiences without crossing into clinical claims territory are exactly the decisions mental health app teams face. We made them on Cultiv8. We know where the lines are and how to build on the right side of them.
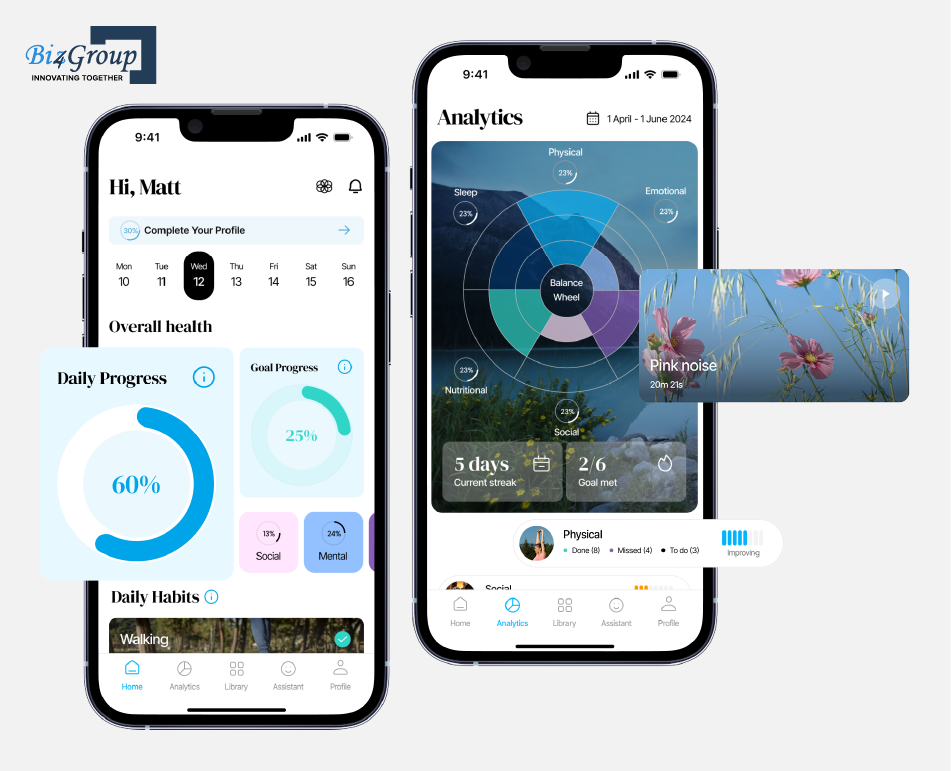
Quantum Fit is an AI-powered personal development platform covering six wellness dimensions: physical, mental, spiritual, nutritional, social, and sleep. The mental wellness layer specifically required us to build AI personalization that felt genuinely responsive to the user's state without making clinical claims about any of the dimensions it tracked.
That is the exact architectural tension teams building AI mental wellness monitoring tools face every day. How do you make the AI feel smart and personal without the language or logic crossing into regulated territory? We built that balance into Quantum Fit and the same thinking applies directly to mood tracking feature design.
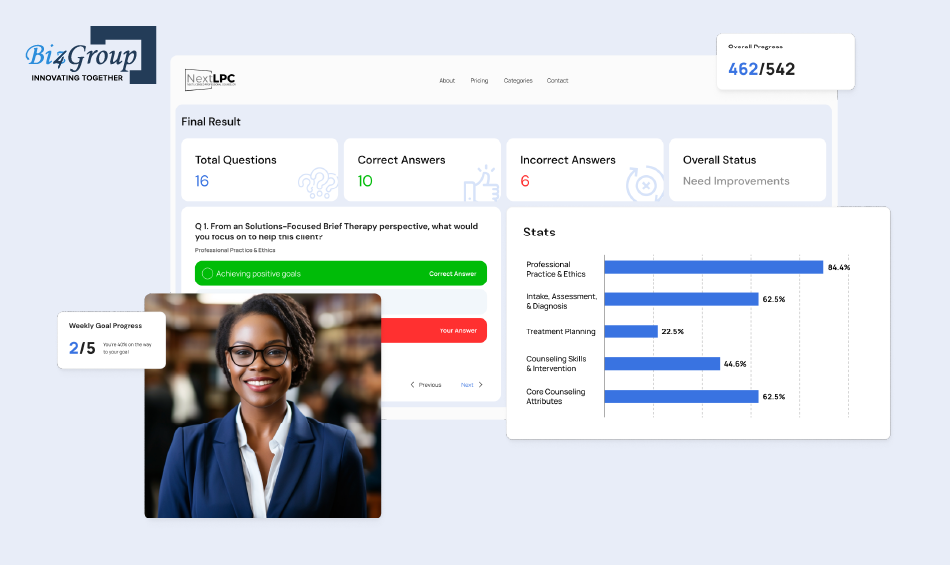
NextLPC is an AI-powered eLearning platform for psychotherapy students. We built AI avatars that act as therapy tutors, guiding students through clinical case studies and licensing exam preparation.
This was not a consumer wellness app. It required our team to understand how therapy frameworks translate into AI behavior, how clinical knowledge gets encoded into an AI system responsibly, and how to build AI that operates correctly inside a mental health professional context. That exposure to the intersection of AI and clinical mental health practice is something very few development firms can claim. It directly informs how we approach AI-based mood tracking and clinical assessment in mental health apps for our clients today.

AI Wizard is an avatar-based AI companion platform where we built conversational AI with real-time adaptive responses. The AI reads context, adapts its behavior dynamically, and maintains coherent conversations across sessions.
The same conversational AI architecture that powers AI Wizard sits underneath mood companion features, adaptive check-in flows, and the escalation logic that mental health apps need to handle responsibly. When a mental health platform needs an AI that responds differently based on a user's current emotional state, routes to crisis resources when needed, or adapts its therapeutic content delivery over time, the engineering foundation is exactly what we built here.
What founders building AI-powered mood analytics in mental health apps get when they work with us is a team that has already solved the component problems. Wellness data architecture. Clinical AI context. Adaptive conversational AI. Personalization without clinical overreach.
We bring those capabilities together with the regulatory knowledge this guide has laid out, the 2026 FDA guidance updates, the classification framework, the PHQ-9 and GAD-7 implementation decisions, the HIPAA architecture, and the compliance documentation that enterprise buyers and investors ask for.
We are an agentic AI development company that has earned the trust of 500 plus clients across healthcare, wellness, and AI. If you are building AI mood tracking in mental health apps with FDA compliance considerations and want a team that understands both the product and the environment it sits in, the conversation starts here.
Let's build it right from day one.
20 plus years. 1,000 plus projects. Zero compliance retrofits for teams that came to us first.
Contact UsThe regulatory landscape for AI mood tracking in mental health apps is not going to get simpler. The FDA is drawing sharper lines. The FTC is actively enforcing. Enterprise buyers are asking mental health app mood tracking compliance questions in the first meeting. Team building without a clear classification decision, documented wellness rationale, and compliant architecture are accumulating risk with every sprint they ship.
But here is what this guide should also make clear: the 2026 updates are not a wall. For teams that make deliberate decisions early, the path is more clearly defined than it has ever been. General wellness builders have more protection. Reimbursement pathways that did not exist two years ago are now open. And clinically validated AI mood tracker products built with credibility from day one are the ones winning the enterprise contracts everyone else is losing.
The difference between those two outcomes almost always comes down to one thing: the decisions made before the first line of code was written.
At Biz4Group, that is exactly where we start. With 20 plus years of experience, 300 plus professionals, and a portfolio spanning wellness AI, clinical mental health platforms, and adaptive conversational AI, we bring regulatory thinking, architecture decisions, and AI mental health app clinical validation documentation into the build process from day one, not as a retrofit when a problem surfaces.
If you are building AI mental health applications for monitoring mood and emotional wellness and want a team that has already solved the hard problems, we are ready when you are.
Your next enterprise contract is waiting on a compliance decision you have not made yet. Let's make it.
Not automatically. The FDA does not regulate your technology; it regulates your intended use. An AI mood tracking in mental health apps feature that helps users reflect on their emotional patterns without making clinical claims generally falls under general wellness enforcement discretion. The moment your app claims to diagnose, treat, monitor, or prevent a specific mental health condition, it likely becomes a Software as a Medical Device requiring FDA clearance. The January 2026 FDA guidance update made this distinction clearer than it has ever been, but the line is still drawn by what you say your app does, not what it technically does.
SaMD is software intended to fulfill a medical purpose such as diagnosing or treating a condition. A general wellness app promotes healthy habits and emotional wellbeing without clinical claims. For AI mood assessment in mental health applications, the distinction comes down to one thing: claims language. "Track how you feel today" is wellness. "Monitor your depression symptoms" is SaMD. The same underlying AI, two different regulatory categories, based entirely on how the product is described across every touchpoint including your App Store listing, onboarding, push notifications, and marketing copy.
Yes, in most cases. Health coaches, wellness practitioners, and app developers can administer PHQ-9 and GAD-7 as self-reflection tools without triggering FDA oversight, provided scores are displayed without clinical interpretation and no treatment recommendations are generated from them. The compliance line is crossed when your AI interprets those scores to produce clinical recommendations, route users to specific treatments, or flag a diagnosis. One non-negotiable regardless of classification: PHQ-9 Item 9, which screens for suicidal ideation, must trigger an immediate display of crisis resources including the 988 Suicide and Crisis Lifeline when endorsed by any user.
It depends on your business model and data flows. HIPAA applies when your app qualifies as a covered entity or business associate handling Protected Health Information. Many consumer wellness apps are not covered entities. However, HIPAA obligations are triggered the moment your mood tracking data connects to a licensed provider, flows into an EHR, or gets processed by a third-party vendor without a signed Business Associate Agreement. Even if HIPAA does not apply, the FTC Health Breach Notification Rule covers many non-HIPAA health apps and carries independent enforcement risk. BetterHelp paid $7.8 million and Cerebral paid over $7 million; neither case was an FDA issue.
For a 510(k) submission, the FDA expects two types of validation. Analytical validation confirms your algorithm measures what it claims to measure, with documented accuracy, sensitivity, and specificity across diverse demographic groups. Clinical validation demonstrates that the AI's outputs lead to meaningful clinical outcomes, using condition-specific endpoints like PHQ-9 or GAD-7 score improvements. The FDA's December 2025 Real World Evidence guidance also encourages planning data collection during development rather than after. If your AI mental health app clinical validation involves an adaptive AI that learns from user data, a Predetermined Change Control Plan must be filed before deployment.
The consequences come from multiple directions simultaneously. The FDA can issue warning letters, require product recalls, or pursue injunctive action for uncleared SaMD. The FTC can pursue enforcement for unsubstantiated clinical claims regardless of FDA classification. State attorneys general are actively enforcing mental health data protection laws in California, Washington, Nevada, and Texas among others. Enterprise buyers will walk away from any vendor that cannot produce a compliance summary. And product liability courts, as signaled by the Garcia v. Character Technologies case in 2024, can attach duty of care to AI mental health tools regardless of their regulatory classification. Misclassification is not just a regulatory risk. It is a commercial one.
Start by asking three questions: Can they explain the difference between the FDA's 2026 General Wellness guidance and SaMD classification in plain language? Have they implemented PHQ-9 and GAD-7 in a clinical context, and do they know what Item 9 requires? Can they describe what a Predetermined Change Control Plan is and why an adaptive AI needs one? A partner who cannot answer these questions clearly is learning on your budget. The right AI mood tracking app development partner brings classification decisions, claims architecture, HIPAA data design, and compliance documentation into the build process from day one, not as an afterthought when an enterprise buyer or regulator asks the question.

with Biz4Group today!
Our website require some cookies to function properly. Read our privacy policy to know more.