info@biz4group.com
info@biz4group.com 





























Imagine a digital system that doesn’t wait for instructions but instead, understands your business goals, learns from real-time feedback, and takes independent actions to get the job done.
Read More

 AI Summary Powered by Biz4AI
AI Summary Powered by Biz4AI
Disclaimer: This blog is for informational purposes only and does not constitute legal, regulatory, or compliance advice.
You didn't wake up one morning and decide to roll out AI without a plan. It probably happened in pieces.
Radiology started using an AI tool to flag scans faster. Scheduling brought in something smarter to cut no-shows. Someone on the clinical side started piloting an ambient scribe because documentation was burning everyone out.
Each decision made sense on its own. But here's the question that actually matters: if someone asked you right now who owns AI governance in healthcare at your organization, would you have a real answer? Or would you be pointing at three different departments and hoping one of them says yes?
You're not alone if you're hesitating. A recent industry analysis found that AI adoption across health systems has hit 75%, but only 18% of those organizations actually have a formal governance structure behind it. That's a massive gap between "we're using AI" and "we know exactly how we're using it, and we can prove it."
It gets more specific too. A late-2025 survey of 182 hospital leaders found that only 22% felt highly confident they could produce a complete AI audit trail within 30 days if a regulator or payer asked for one. Among smaller hospitals, that confidence dropped to just 15%. If you were asked that question tomorrow, would your team be in the confident group, or the other one?
Here's what makes this moment different from past tech rollouts. You're not just managing software anymore. You're managing systems that touch patient charts, influence clinical decisions, and create new categories of risk that HIPAA and FDA rules were never written with in mind.
We've worked as an AI healthcare software development company long enough to see where governance gaps actually show up. It's rarely the tools themselves that cause problems. It's the space between adoption and oversight, where decisions get made fast and documentation gets written later, if it gets written at all.
This guide is built to close that gap. We're going to walk through how to implement AI governance in healthcare for risk, bias, and compliance management, how AI governance in healthcare organizations actually overlaps with the regulations you already answer to, how to keep generative AI from quietly creating risk in patient charts, and how to measure whether any of this is genuinely working once it's in place.
No theory for theory's sake. Just what you need to build a healthcare AI governance framework your compliance team, your clinicians, and your patients can actually trust.
Let's start with an honest question. When your radiology team adopted an AI tool, did legal sign off on it? Did anyone test it against your actual patient population before it went live? If the answer is "not really," you're not alone, but you are exposed.
This is the part most healthcare leaders get wrong about AI governance in healthcare. They treat it like a compliance checkbox you get to later, once the budget allows or once something forces the issue. Before we go further, it's worth settling what this term actually means, because most of the confusion in healthcare boards and leadership meetings starts right here.
AI governance in healthcare is the set of people, processes, and decision points that determine whether an AI tool is safe enough to touch patient care, and whether it stays that way after launch. That's the whole definition. Notice what's missing from it: a policy document.
You can have a beautifully written AI policy sitting in a SharePoint folder that nobody reads and still have zero actual governance happening on the floor. A policy is a statement of intent. Governance is the machinery that makes the statement true.
Real governance in an AI governance in healthcare system means something is actively watching. It means a defined group of people approves new AI tools before they touch patient care, not after a department has already started using one. It means someone is tracking how those tools perform after launch, not just at the pilot stage. And it means a nurse or physician who notices something off has a clear path to flag it, and that flag actually goes somewhere instead of sitting in an inbox.
If you're building this for the first time, the smartest place to start isn't the framework itself. It's a step earlier than that. Working through a list of questions to ask before AI adoption in healthcare before a tool ever reaches a pilot stage will tell you more about what your governance program needs to cover than any template will.
Once you've got that working definition in your head, the next part makes a lot more sense. Here's why the gap between adopting AI and governing it isn't just an oversight problem. It's already shaping what happens to your patients.
Ungoverned AI doesn't fail loudly. It fails quietly, in small inconsistencies that look like noise until you connect the dots.
A scheduling algorithm that deprioritizes certain zip codes. A diagnostic tool that performs well in trials but stumbles on patients outside the dataset it was trained on. A documentation assistant that smooths over a detail a clinician would have caught.
None of these show up as a single dramatic failure. They show up as a slow erosion of trust and accuracy, and by the time someone notices, the tool has likely been making those calls for months.
This is why AI ethics and governance can't sit in a binder waiting for an annual audit. The whole point of governance is catching these patterns while they're still small. Without it, you're not avoiding risk. You're just delaying the moment you find out about it, and that delay gets paid for by a patient, not a spreadsheet.
Think about what happens when a retail recommendation engine gets something wrong. Someone sees an ad they didn't want. Annoying, but recoverable.
Now think about what happens when a clinical AI tool gets something wrong. A missed flag on a scan. A biased risk score that deprioritizes a patient who needed urgent care. There's no "we'll fix it in the next release" in that scenario.
And the risk here isn't theoretical. A systematic review covering ten years of data found a clear association between AI use in healthcare and a worsening of racial and ethnic disparities in patient outcomes, largely because the algorithms were trained on data that already carried those imbalances forward. That's not a hypothetical edge case. That's what happens when AI governance improvement gets treated as a someday project instead of a now one.
This is what separates AI in healthcare governance from governance in almost any other sector. You're not protecting revenue or brand reputation as the primary goal, even though both matter. You're protecting people who had no say in which AI tools your organization chose to deploy. That's a different kind of responsibility, and it deserves a different level of rigor.
Over 80% of physicians are now using AI in their day-to-day work, and most of that adoption is moving faster than the governance behind it.
Talk to Our Healthcare AI TeamStrip away the consultant language and building AI oversight frameworks in healthcare comes down to four working parts. Miss any one of them and the rest stops functioning. Here's what actually has to be in place, and who's responsible for each piece.
You need representation from clinical leadership, IT, compliance, legal, and data science, even if that last seat is filled by a contracted resource. No single department should have the power to approve an AI tool alone. This is the foundation every other piece of AI governance in healthcare organizations rests on.
Every tool needs an intake process before it touches patient care. That means a risk assessment, a check against your existing data and patient population, and a documented decision, approved, piloted, or rejected. Skip this step and you're governing reactively instead of proactively.
Decide your performance and safety thresholds before a tool goes live, not after something goes wrong. These thresholds tell you exactly when to pause, retrain, or pull a tool entirely. This is one of the clearest AI governance best practices for hospitals, and it's the one most frameworks skip.
Most of your AI exposure comes from vendors, not internal builds, so your healthcare AI governance framework has to cover tools you don't fully control. That means contract language on liability, validation requirements before go-live, and ongoing access to performance data, not just a sales demo and a signature.
A solid AI governance platform ties these four pieces together so they function as one system instead of four disconnected checklists.
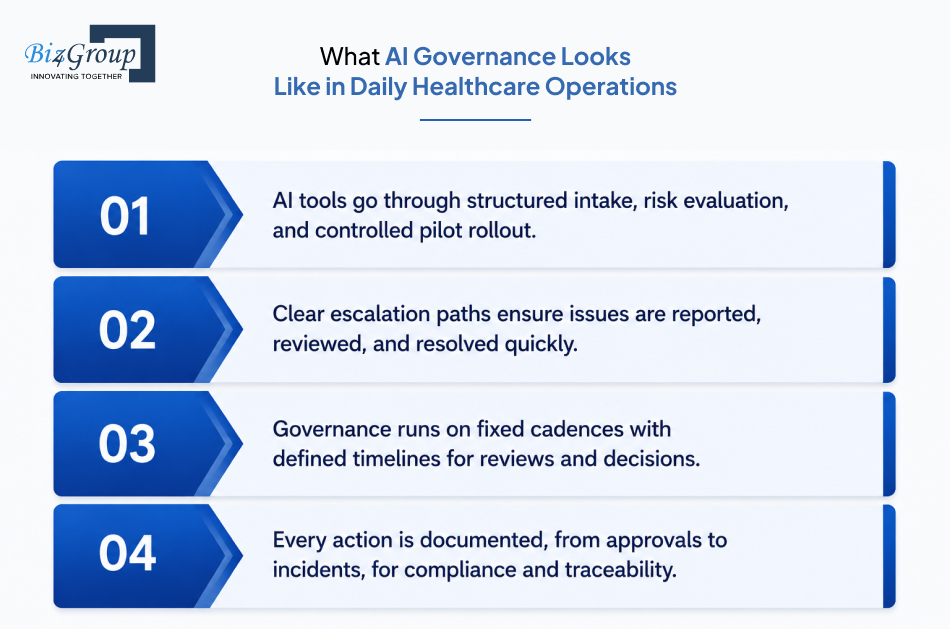
It's easy to talk about governance in the abstract. It's harder to picture what it actually looks like once it's running inside a healthcare organization, day to day, tool to tool. So, let's walk through it. This is how to implement AI governance in healthcare for risk, bias, and compliance management actually looks like once it's no longer just a document sitting in a folder.
A department wants to bring in an AI tool, it could be in imaging, billing, staffing, documentation, or anywhere else patient or operational data is involved. Before it touches a live workflow, it goes through intake, gets evaluated against your existing thresholds, and either gets approved for a limited pilot, sent back for more validation, or rejected outright.
Governance only works if the people closest to patient care can flag a problem and know it'll actually be addressed. A clinician noticing inconsistent AI output shouldn't have to guess who to tell or whether it's worth the effort. That path needs to be short, clear, and the same every time, which is exactly what good AI governance policies for clinical AI applications and patient safety are designed to guarantee.
Most frameworks fail here, not because the structure is wrong, but because meetings stop happening once the initial excitement wears off. A working AI governance in healthcare organizations program needs a fixed cadence, plus a lighter process for anything urgent that can't wait for the next scheduled meeting.
If a regulator, payer, or legal team ever asks how a specific AI-influenced decision was made, you need to answer that question with records, not memory. This is what creating AI oversight frameworks in hospitals to ensure safe and ethical deployment actually means in practice, and it's what separates a real healthcare AI governance framework from one that only exists on paper.
Tools that bring AI healthcare workflow automation into this process make a real difference here, since manual tracking across departments is exactly where governance tends to quietly fall apart.
If you've ever sat in a meeting where someone cites HIPAA, someone else cites the FDA, and a third person mentions a state law nobody's read in full, you know the confusion this section is meant to fix. This is where implementing ethical and regulatory AI governance frameworks for healthcare providers really get tested, because the rules don't live in one place. Let's separate what's actually required from what's good practice dressed up as law.
HIPAA doesn't have an "AI clause." It applies to your AI tools the same way it applies to any system touching protected health information, through the Privacy Rule and Security Rule. If an AI vendor processes PHI, you need a signed Business Associate Agreement, and you need to know exactly where that data goes, including whether it leaves your infrastructure to reach a third-party model.
This is the part that catches organizations off guard. Many assume that because a tool is "just" summarizing notes or scheduling appointments, HIPAA doesn't apply strictly. It does. Any system touching PHI needs the same scrutiny, which is exactly why HIPAA-compliant AI healthcare software has to be built with this in mind from day one, not patched in after deployment.
Is your AI tool secretly a medical device? If it's making or influencing a diagnosis, treatment recommendation, or clinical decision, there's a real chance it qualifies as Software as a Medical Device, and that changes everything about how it needs to be validated and monitored.
The FDA's oversight here isn't shrinking. As of the first quarter of 2026, the agency had authorized 1,524 AI-enabled medical devices since it began tracking them in 1995, with 92 new authorizations added in that quarter alone. If your tool falls into SaMD territory and hasn't gone through that process, you're carrying risk that has nothing to do with HIPAA at all, and this is the exact gray zone where building AI compliance strategies in healthcare systems to meet regulatory requirements has to start early instead of after a vendor contract is already signed.
While HIPAA and FDA rules sit at the federal level, states aren't waiting around. More than 250 AI-related healthcare bills have been introduced across 34 states as of early 2026, covering everything from bias audits to disclosure requirements when AI is used in patient interaction.
This matters more than it sounds. A tool that's fully compliant federally can still put you out of step with a requirement specific to your state, and that gap is exactly where AI governance in healthcare organizations programs need a standing process for tracking legislative changes, not a one-time legal review.
When you're briefing leadership, it helps to separate what you're legally obligated to do from what's simply smart practice. This is also a useful gut check on whether your current AI governance in healthcare system is built around actual obligations or just borrowed best practices from another industry:
Treat the recommended column seriously anyway. Regulation in this space moves fast, and what's optional today tends to become required within a year or two.
Let's figure out exactly where your AI program sits on the compliance map before a regulator does it for you.
Get a Compliance Gap CheckYou can have a governance committee, a charter, and a stack of approved policies, and still have no real AI governance improvement happening on the ground. This is the exact question a lot of digital health leaders quietly struggle with: how to actually measure whether our AI governance program is working or if it's just documentation that nobody follows in practice. The honest test isn't whether the documents exist for your AI governance in healthcare program. It's whether anyone's actually following them when nobody's checking.
A policy that says clinicians must report unusual AI output means nothing if staff don't know the policy exists, or know it but don't trust that reporting changes anything. The real signal isn't the document. It's whether people act on it without being reminded.
Ask yourself something simple. If you pulled ten staff members at random and asked them how to flag a problem with an AI tool, would they know? If the answer is no, the policy is decoration, not governance.

Plenty of organizations track metrics that look productive but don't say much. Number of policies written. Number of training sessions held. This tells you effort happened, not whether it worked.
Better metrics look like this:
This is the kind of detail that separates best practices for healthcare AI compliance and governance programs that function from ones that just look good in a board deck. It's also where AI tools for data governance in healthcare earn their value, since manually pulling this kind of evidence together across departments is where most internal efforts quietly stall out.
You don't need an external audit to get an honest read on where you stand. A short internal check, scored across a few categories like committee activity, intake consistency, monitoring frequency, and documentation completeness, will usually reveal the gap fast. This kind of self-check is part of what real AI governance best practices for hospitals look like once they move past the policy stage.
Budgets are starting to reflect this shift too. Among hospitals surveyed heading into 2026, only 26% planned to raise their AI governance and safety budget by two or more percentage points, while 18% planned no increase at all. If your organization is in the "no increase" group while your AI footprint keeps growing, that mismatch is worth flagging to leadership directly.
There's no shame in admitting your internal team doesn't have the bandwidth or specialized expertise to run this well on top of everything else they're already doing. Most healthcare organizations don't, and trying to force it internally often costs more in rework than bringing in the right partner from the start.
Before that conversation happens, it helps to have a realistic sense of the cost of implementing AI in healthcare governance work specifically, separate from the cost of the AI tools themselves. Leadership tends to underestimate this line item until it's already overdue.
Ambient scribes solve a real problem. Documentation burden is one of the biggest drivers of clinician burnout, and a tool that listens to a visit and drafts the note sounds like an easy win. It mostly is, until it isn't, and that's where generative AI governance in healthcare earns its place as its own dedicated conversation, not a footnote inside your broader framework.
Most existing governance frameworks were designed around predictive AI tools that flag a risk score or sort a worklist. Generative AI doesn't just flag something. It writes something, in natural language, that looks exactly like a clinician's own documentation. That difference matters more than it sounds.
Even leading ambient scribe systems carry a hallucination rate of roughly 1 to 3 percent on clinical content, and research has found that physical examination findings are among the highest-risk areas, with some systems documenting exam details that never actually happened during the visit. A 1 to 3 percent error rate sounds small until you multiply it across thousands of patient encounters a month.
If you're using generative AI for clinical documentation and ambient scribing, you've probably had the same worry a lot of digital health leaders bring to us: hallucinated notes ending up in patient charts, and what governance controls actually prevent this. The answer isn't one control. It's a layered one, built directly into your AI governance policies for clinical AI applications and patient safety:
Skip the review step to save time, and you've quietly removed the one control that actually catches the error before a patient's permanent record absorbs it.
Ambient scribes record conversations, and that recording often lives in cloud infrastructure separate from your EHR. Patients deserve clear answers about where that audio goes, how long it's retained, and who can access it beyond the care team in the room.
This overlaps directly with how you handle PHI data architecture more broadly, since a recorded clinical conversation carries the same sensitivity as any other protected health information, regardless of the format it's stored in.
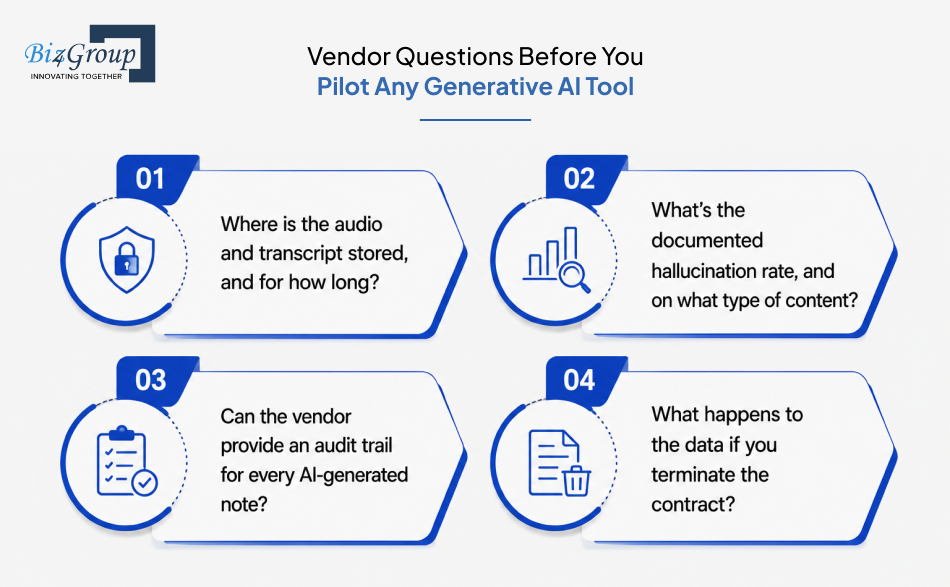
Before a generative AI tool gets anywhere near a live patient encounter, your team needs straight answers on a few things:
A vendor that can't answer these clearly isn't ready for your patients yet, no matter how polished the demo looks.
Most vendors will tell you their model is fair. Most internal teams will tell you they tested for bias. And most of the time, neither claim has been verified the way it should be. This is the uncomfortable part of AI ethics and governance that a lot of organizations would rather not dig into, because the answers aren't always flattering.
A 2025 analysis of over 1.7 million AI-generated clinical recommendations across nine different models found that patients identified as Black or unhoused were more likely to receive recommendations for urgent care, mental health referrals, or invasive interventions than patients with identical clinical presentations. The clinical facts were the same. The recommendations weren't. Here's where that kind of bias enters, how to catch it without a data science team, and what should happen once you do, all in one place.
Where Bias Enters |
What It Looks Like in Practice |
How to Test for It (No Data Science Team Needed) |
What Should Trigger Real Action |
|---|---|---|---|
Training data |
Model learned from a patient population that doesn't reflect yours |
Compare the vendor's validation demographics against your own patient mix before go-live |
If the gap is significant, require local validation before approval, not after |
Deployment drift |
Performance was fine at launch, degrades as your patient mix shifts over time |
Re-run the same subgroup comparison on a fixed schedule, not just once at launch |
Repeated drift across cycles means the tool is paused for retraining or revalidation |
Proxy variables |
Model uses cost, zip code, or insurance type as a stand-in for medical need |
Check which input variables most heavily influence the output, even ones that look neutral |
If a proxy variable is driving the gap, it gets removed or reweighted before redeployment |
Sociodemographic inputs |
Recommendations shift based on race, housing status, or other patient demographics |
Run identical clinical cases through the tool, varying only the demographic detail |
Any outcome gap that clinical factors alone can't explain pauses that use case for review |
Thin subgroup data |
No bias detected, but data for a specific subgroup is too sparse to trust the result |
Flag subgroups where your sample size is too small for a confident result |
Tool stays under expanded monitoring instead of getting a clean pass |
This is exactly the kind of structured testing that AI tools for data governance in healthcare are built to support when your organization doesn't have specialized staff in-house to run it manually, and it's the foundation behind creating AI oversight frameworks in hospitals to ensure safe and ethical deployment that actually catch problems instead of just documenting them after the fact.
One more thing, the table doesn't fully capture. The more autonomy you hand an AI tool, the more deliberate your human checkpoints need to be, especially as healthcare moves toward more independent, agentic AI in healthcare systems that can take multiple steps without a person prompting each one. For anything touching diagnosis, treatment recommendations, or care prioritization, a clinician needs to see and approve the call before it affects the patient, every time, with no exceptions carved out for convenience.
There's a difference between a company that talks about AI governance and one that's actually had to build inside its constraints. At Biz4Group, governance isn't a slide we add to a proposal after the technical work is scoped. It's part of how we architect the system from the first conversation, because we've seen what happens when it's bolted after the fact.
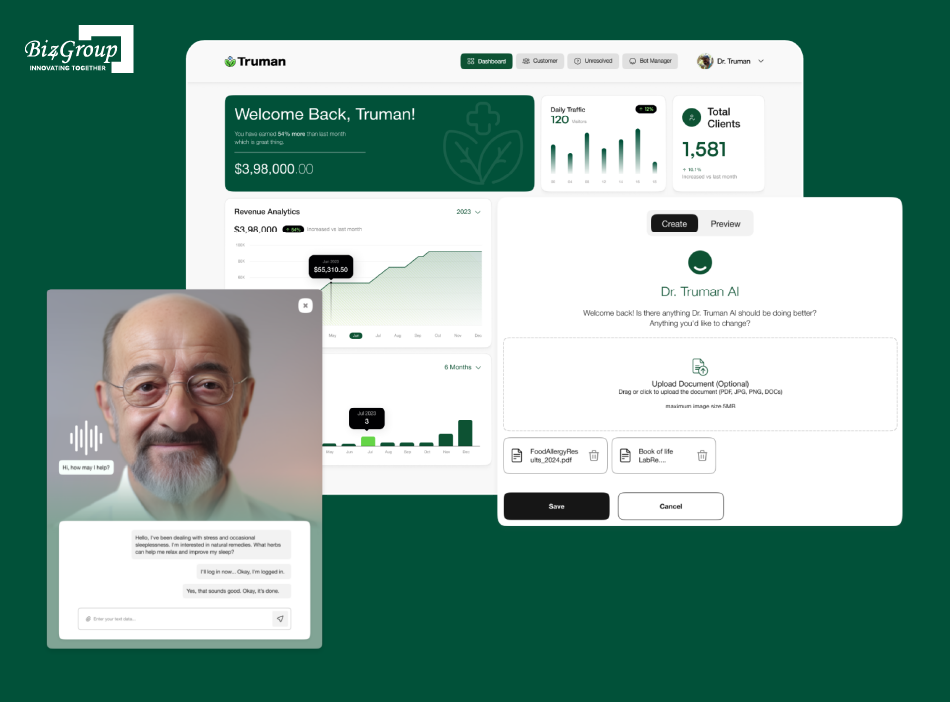
Take our work on Dr. Truman, an AI-powered healthcare platform built around an interactive avatar that personalizes care experiences for patients. Getting that platform right meant something most demos skip over entirely. Responses were developed in collaboration with clinical experts and reviewed for accuracy before reaching patients, because a friendly interface doesn't excuse an unverified clinical answer. Patient data protection was treated as a core requirement from day one, not a feature added once the platform started scaling.
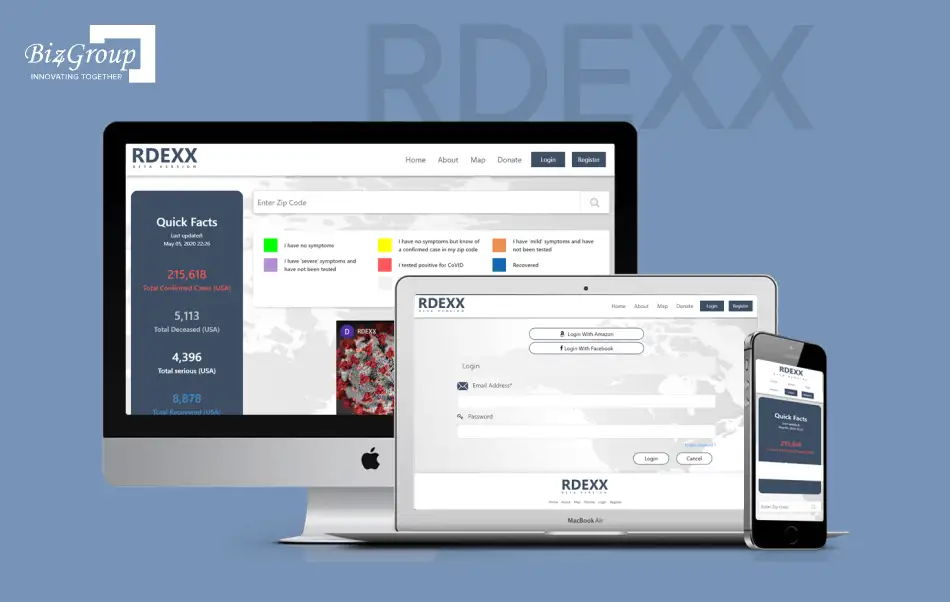
That same discipline shaped RDeXX, an AI-powered telehealth intelligence platform built for global health preparedness, with color-coded severity indicators and live data integrations that healthcare teams could trust to act on quickly, often across borders and under real time pressure. Building something hospitals and health networks rely on for fast, accurate decisions means the underlying governance can't be an afterthought. It has to hold up the moment something urgent happens.
We've also built custom enterprise AI agent systems for large healthcare organizations looking to bring more autonomy into operational decision-making. The more independently a system can act, the more deliberately it needs to be governed, and that principle shows up in every project we take on, not just the ones labeled "agentic."
This is the kind of question we hear before a project even starts, usually from someone running compliance at a regional hospital system already using AI across a couple of departments: "we do not have a formal governance framework in place and I want to know what an actual AI governance structure should look like for a healthcare organization our size." We don't hand over a template to answer that. We start by understanding the size, specialty mix, and existing AI footprint of the organization, because a framework built for a five-hospital regional system looks like nothing one built for a single community hospital.
Here's what carries across all of it. Every healthcare project we build is approached with HIPAA, FDA, and broader regulatory alignment baked into the architecture, not retrofitted after launch. That's the only way to build something a compliance officer, a clinician, and a patient can all trust at the same time, and it's why healthcare organizations keep coming back to us when the stakes are too high for a vendor who's only building for the demo.
If you're evaluating partners for your own AI healthcare governance framework, ask them what happened the last time something didn't go as planned in a healthcare build. The answer tells you more than any pitch deck will.
Let's design a system that's governed from the first line of code, not patched after the fact.
Start the ConversationIf there's one thing worth carrying forward from everything we've covered, it's this. AI governance in healthcare isn't a phase you complete and move past. It's a discipline you keep practicing as your tools, your patient population, and your regulatory landscape keep shifting under you.
Structure without enforcement is decoration. Compliance without monitoring is a false sense of safety. And bias testing without real consequences is just a report nobody reads twice. Put together properly, these pieces give you a real healthcare AI governance framework, one you can actually defend, to a regulator, to your board, and to the patients trusting you with their care. That's what separates organizations with genuine AI governance in healthcare organizations maturity from the ones still operating off a binder nobody's opened since the audit.
We've built inside these exact constraints across real healthcare platforms, not just written about them, which is the difference between advice that sounds right and advice that's been tested under pressure. If you're building or refining your own healthcare software product, that experience is exactly what shortens the distance between "we have a policy" and "we have a program that works."
Your AI tools aren't waiting for a governance framework to catch up. They're already making decisions today. The only real question left is whether you're steering that, or just watching it happen.
There's no single owner. AI governance in healthcare organizations works best as a shared responsibility across a multidisciplinary committee that includes clinical leadership, IT, compliance, legal, and data science. If one department holds all the decision-making power, you've created a blind spot, not a real AI governance in healthcare system.
Governance is the internal structure, your committees, intake process, and monitoring routines. Compliance is the external proof that this structure actually satisfies HIPAA, FDA, and state requirements. You can't be compliant without building AI oversight frameworks in healthcare behind it, but a committee that meets without producing documentation isn't compliant governance either. It's just a meeting.
Some of it is legally required, and some of it isn't, which is exactly why this confuses so many compliance teams. HIPAA and FDA obligations apply whenever your AI tools touch PHI or qualify as a medical device. Implementing ethical and regulatory AI governance frameworks for healthcare providers beyond that, like voluntary alignment with NIST's AI Risk Management Framework, often backfires when treated as optional, since more than 250 AI-related healthcare bills are already moving through 34 states.
In most cases, liability falls on the hospital and the treating physician, not the AI vendor, regardless of how the tool was marketed. This is precisely why AI governance policies for clinical AI applications and patient safety need to require independent clinical judgment on every AI-assisted decision, since that judgment is your strongest defense if an outcome is ever questioned.
Document the clinical reasoning behind the decision, not just the AI tool's output. A note that shows a clinician reviewed, questioned, or confirmed by an AI recommendation demonstrates independent judgment. This kind of documentation discipline is one of the simplest AI governance best practices for hospitals, yet it's the one most team only think about after something's already gone wrong.
Most healthcare systems run a full committee review monthly or quarterly, with a smaller subgroup available to handle anything urgent between those meetings. The exact cadence matters less than consistency, and it's a core part of how to implement AI governance in healthcare for risk, bias, and compliance management in a way that holds up over time. A committee that meets twice and then quietly stops is worse than one that never started, because it creates a paper trail suggesting oversight that wasn't really happening.
AI ethics and governance are related but not identical. Ethics asks whether an AI tool's outputs are fair, transparent, and respectful of patient autonomy. Governance is the operational system that enforces those ethical standards in practice, through approval processes, bias testing, and ongoing monitoring, the same operational discipline behind creating AI oversight frameworks in hospitals to ensure safe and ethical deployment. Ethics sets the standard. Governance is what actually holds you to it.

with Biz4Group today!
Our website require some cookies to function properly. Read our privacy policy to know more.