info@biz4group.com
info@biz4group.com 





























Imagine a digital system that doesn’t wait for instructions but instead, understands your business goals, learns from real-time feedback, and takes independent actions to get the job done.
Read More

 AI Summary Powered by Biz4AI
AI Summary Powered by Biz4AI
What's it actually costing you every time a nurse has to call another department just to confirm something a screen should have shown her already?
If you're running a hospital network and still leaning on a mix of legacy systems and newer platforms, you already know the real cost of that setup. It's not just slow data. It's missed lab results, duplicate imaging, and staff spending their shift chasing information that should already be in front of them.
Sound familiar? You're not alone, and you're definitely not behind in the way you might think.
Here's a number worth sitting with: as of early 2026, only 43% of hospitals engage in all four domains of interoperable health information exchange. That means more than half the country is still working through the exact problem you're facing right now. You're in the majority, not the exception.
And the pressure isn't going away. CMS now requires networks to expose patient data through modern FHIR APIs aligned with USCDI v3 by July 4, 2026. That deadline is closer than it feels.
So where does that leave you? Stuck between a clock that's ticking and a tech stack that wasn't built for this?
We've sat across the table from CTOs and IT directors who inherited this exact mess. Nobody planned it this way. It happened one acquisition, one new specialty system, and one "temporary" workaround at a time. And now leadership wants results without a multi-year rebuild that puts patient care at risk.
Here's the part that should make you feel better: you don't need to rip out your legacy systems to achieve interoperability in healthcare. In most cases, the smarter and faster path is to modernize legacy software in healthcare in stages, while building around the right healthcare interoperability standards and protocols and a realistic view of where most EHR interoperability in healthcare projects actually break.
That's exactly what we're going to walk through. Just what interoperability in healthcare actually means, what the benefits of interoperability in healthcare look like once you get there, where the real obstacles sit, and how to move forward using the systems you already have.
Ready to see what this actually takes? Let's get into it.
Let's start simple. Interoperability in healthcare is the ability for different systems, whether that's your EHR, your lab software, your billing platform, or a hospital across town, to share patient data in a way that's accurate, secure, and usable the moment it arrives.
Not a PDF that someone has to re-read and retype. Not a fax that sits in a queue for three hours. Actual structured data that lands in the right field, in the right chart, ready for a clinician to act on.
That's it. That's the whole idea.
But here's where most explanations stop short, and where they leave CTOs and IT leaders with more questions than answers: interoperability in healthcare isn't one switch you flip. It happens in layers. You can have systems that technically connect but still can't understand each other's data. You can have data that's understandable but still can't be acted on because nobody agreed on the rules for sharing it.
We'll get into those layers in the next section, because understanding them is the difference between guessing at a fix and actually building one.
Here's a question worth asking your own team: how many hours a week does your staff spend tracking down information that already exists somewhere in your network?
If you don't know the answer, you're not alone. Most leadership teams don't, because that time gets absorbed into the workday and never shows up on a report. But the research does show up. Healthcare professionals spend roughly 15% of their workweek searching for patient information outside their core systems, and at any given moment, fewer than 7% of providers have all the patient data they need sitting inside their own EHR.
Sit with that for a second. That's not a small inefficiency. That's nearly a sixth of your clinical and administrative workweek spent chasing data that interoperability in healthcare should be delivered automatically.
So why is interoperability important in healthcare, beyond the obvious answer of "it saves time"? A few reasons that matter more the longer you sit in this industry:
None of this is about chasing technology or checking a regulatory box. It's about whether the people treating your patients have what they need and when they need it. And right now, for most hospital networks, they don't.
That gap is exactly what the rest of this guide is built to close.
Your hospital network shouldn't need a phone tree just to find a lab result. Let's fix that without touching your budget for a full rebuild.
Talk to Our Interoperability TeamBy now you know what interoperability is and why it matters. But if you're the one signing off on the budget, you need more than that. You need to know exactly what you're getting back for the investment.
So, let's break down the benefits of interoperability in healthcare by who actually feels them, because the value shows up differently depending on where you're sitting in the organization.
Clinicians get their time back, and they get a fuller picture of the patient in front of them. Instead of piecing together history from whatever's been manually entered, they're working from a complete, current record pulled through healthcare data interoperability.
Patients get continuity, even when their care doesn't happen in one place. Interoperability in healthcare means their full story travels with them, no matter how many facilities or providers are involved.
Your finance team gets fewer redundant tests, lower administrative overhead, and a real reduction in the staff hours lost to manual data chasing.
Your compliance team gets a much easier audit trail once data interoperability in healthcare replaces manual workarounds with standardized, documented exchange.
Your IT team gets fewer one-off fixes, and less time spent maintaining custom point-to-point connections that break the moment one system gets updated.
Leadership gets a network that's actually easier to grow, since systems built to exchange data cleanly don't require a new layer of custom work every time the organization expands.
We've worked closely with hospital networks and health-tech teams chasing exactly this kind of return, and the pattern is always the same. The wins rarely show up as one big number. They show up as a long list of smaller frictions disappearing across every department, which is why this is hard to justify with a single metric and easy to justify once the full picture is in front of you.
But here's the catch leadership doesn't always see coming. Not every hospital network is starting from the same place, and interoperability in healthcare isn't something you either have or don't. It happens in layers, and most organizations are further behind than they think. So, before you plan your next move, you need to know exactly which layer your systems are actually stuck at right now.
Saying your systems are "interoperable" doesn't mean much on its own, because interoperability in healthcare isn't one thing. It's four distinct layers, defined by HIMSS, and each one solves a different problem. Most hospital networks assume they're further along than they actually are, simply because they've never mapped their systems against all four.
It is the most basic layer. It means one system can send data and another system can receive it, nothing more. A fax machine technically achieves foundational interoperability. So does an email with a PDF attached. The data moves, but the receiving system has no ability to read it, sort it, or act on it without a human stepping in first.
This is the layer where data starts arriving in a standardized format with defined fields, and it's the foundation of real healthcare data interoperability. This is where HL7v2 messaging and FHIR interoperability standards operate. A lab result arrives as a lab result, tagged correctly, landing in the lab section of the chart instead of a scanned document someone has to manually file. The structure is consistent, even if two systems don't fully agree on what every value inside that structure means.
This is where the systems agree on meaning, not just format. This depends on shared coding standards: SNOMED CT for clinical terms, LOINC for lab tests, RxNorm for medications, and ICD-10 for diagnoses. If Hospital A codes a diagnosis using one set of codes and Hospital B's system can correctly map that to its own internal terminology without a human translating it, that's semantic interoperability. This is the layer most legacy systems were never built for, since many older platforms predate widespread adoption of these coding standards, which is exactly why EHR interoperability in healthcare so often breaks at this stage rather than at the connection itself.
This layer is built on policy, not technology. It covers the legal agreements, consent management, governance structures, and trust frameworks, like TEFCA's Common Agreement, that determine whether data is actually permitted to move between organizations, under what conditions, and with whose authorization. A hospital network can have flawless semantic interoperability internally and still fail at organizational interoperability the moment it tries to exchange data with an outside health system operating under different consent rules.
This is the layer where the technical lift is real but solvable, which is exactly why most networks get this far and stop. FHIR interoperability standards and HL7v2 give you a defined message format to build against, so getting data to move in a consistent structure is a project with a clear technical scope and a clear finish line.
Semantic interoperability is a harder problem because it isn't solved once. Every new data source, every new partner system, every acquired clinic potentially brings its own coding conventions, abbreviations, and local terminology quirks that have to be mapped against standard vocabularies. This is where most healthcare system integration and interoperability efforts quietly stall, not because the data won't move, but because nobody owns the job of keeping it meaningful as the network grows.
Organizational interoperability is harder still, because it isn't an IT problem at all. It requires legal teams, compliance officers, and leadership across multiple organizations to agree on data governance terms, which moves at the speed of contract negotiation, not software deployment. A network can be technically capable of semantic-level data exchange and still be blocked from actually exchanging anything, simply because the legal and consent framework with a given partner hasn't been finalized.
Knowing exactly which level your network is stuck at changes what you build next. A network stuck at foundational needs basic structured data exchange before anything else matters. A network stuck at structural needs investment in terminology mapping and healthcare interoperability standards and protocols, not new hardware. A network stuck at semantic needs governance work, not more engineering.
Knowing which level you're stuck at is half the battle. We'll help you figure out the rest, and actually move up a level.
Get a Free Interoperability AssessmentDefinitions and standards only get you so far. At some point you need to see what this actually looks like when it's working, because that's what turns an abstract concept into something you can point to and say; that's the version we're building toward. Here are three real examples of interoperability in healthcare operating at scale right now.
CommonWell Health Alliance, a Qualified Health Information Network under TEFCA, now supports data exchange for over 261 million patients across more than 125,000 provider organizations in the US. That means a provider using one EHR vendor can run a single query and pull a patient's records from a completely different vendor's system, without a phone call, a fax, or a manual records request.
This works because CommonWell became a Carequality implementer, connecting two of the country's largest health information exchange frameworks so that a hospital running Cerner, Meditech, or athenahealth can retrieve records from a provider running Epic, and vice versa. A nurse practitioner at Lafayette General Health described the practical effect of this directly: it lets her quickly answer the question she asks nearly every patient in urgent care, whether they've had any recent visits to other facilities, and build a treatment plan around the answer instead of around a guess.
Under the CMS Interoperability and Patient Access rule, Medicare Advantage and Medicaid plans were required to launch patient-facing APIs built on FHIR interoperability standards, giving patients programmatic access to their own medical history, lab results, and treatment plans through any app of their choosing. Instead of logging into five different patient portals for five different providers, a patient's data becomes something their own chosen health app can pull directly, on demand.
This same FHIR-based approach is what powers automated provider-payer data exchange for the CMS prior authorization rule, where instead of a clinic faxing a request and waiting days for an answer, the authorization status moves between provider and payer systems through a standardized API call.
The UK's NHS offers one of the clearest large-scale examples of what happens when an entire health system commits to one interoperability standard. As of 2026, numerous NHS suppliers have updated their products to be FHIR-compatible, and the NHS has published an API gateway and catalogue where most APIs follow the FHIR standard, with programs like GP Connect using it specifically to share general practitioner records across other providers. The result is a patient who moves between NHS regions or care settings without their record needing to be rebuilt from scratch at every stop, because every connected system already speaks the same structured language.
What ties all three examples together is the standard underneath them. Every one of these only works because the systems involved agreed to speak FHIR, which is exactly why the next section is worth slowing down for if you're the one deciding what your own network builds on.
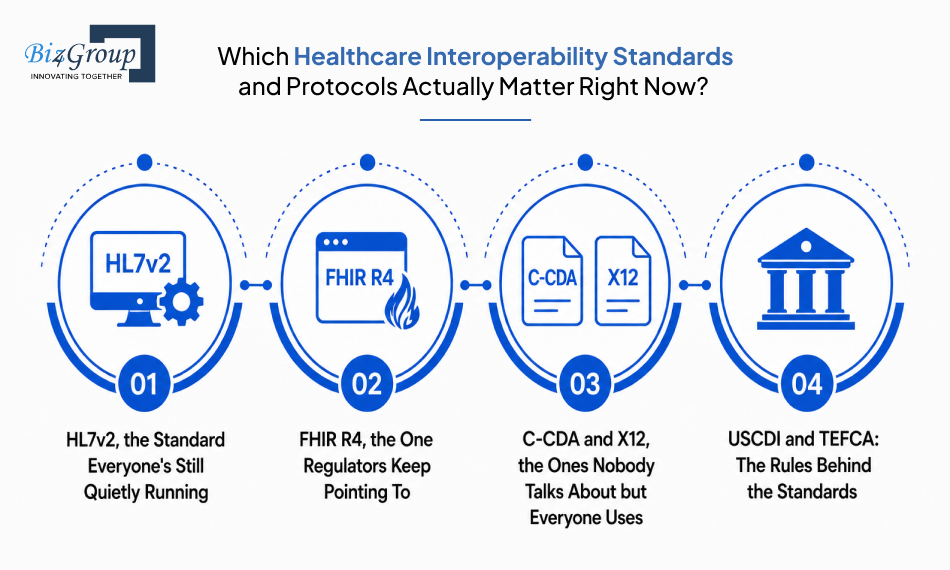
Knowing the four levels of interoperability is one thing. Knowing which standards actually get you there is the next piece, because every one of these levels depends on a specific protocol doing the work underneath it. Here are the healthcare interoperability standards and protocols that matter most to a hospital network in 2026, and where each one actually fits.
HL7v2 is the messaging standard most legacy hospital systems were built on, and it's still moving the bulk of lab, admission, and discharge data behind the scenes today. It works, but it allows so many optional fields and local variations that two systems claiming to be HL7v2 compliant often still need custom interface mapping to understand each other. This is usually the layer responsible for the most fragile, hardest-to-maintain connections in a hospital network's stack, and it's a major reason EHR interoperability in healthcare breaks down at the integration point rather than at the data itself.
FHIR interoperability standards are built specifically for web-based, API-driven data exchange, using REST APIs and JSON instead of rigid message formats. It's the standard ONC, CMS, and TEFCA all point to for new certified health IT, patient access APIs, and prior authorization exchange. Unlike older standards, FHIR breaks data into discrete, reusable resources, so a system can pull up just the medication list it needs instead of an entire document. If you're planning any new healthcare system integration and interoperability work in 2026, this is the standard to build it on.
C-CDA is the document-based standard used for discharge summaries, referral notes, and care summaries. Anywhere a full clinical narrative needs to move as one package rather than as discrete data points. X12 handles administrative and financial transactions, including claims, eligibility checks, and remittance, and it's still the backbone of most payer-facing healthcare data exchange interoperability. Most hospital networks run both alongside FHIR rather than choosing one over the other, since each handles a different category of data, and getting this mix right is usually a core part of any serious healthcare software product development effort.
USCDI is the standardized set of data classes that defines exactly which information must be shared, things like medications, lab results, and clinical notes, so every certified system is working from the same expected data set. TEFCA is the governance layer on top of all of it, the framework that determines who can request and exchange that data, under what terms, across a nationwide network of Qualified Health Information Networks. Together, they answer the two questions that standards alone can't: what has to be shared, and who is allowed to ask for it.
Knowing these standards by name is useful. Knowing how to actually build with one of them, especially the one regulators keep circling back to, is where the real decisions start. That's exactly where we're headed next.
FHIR interoperability standards organize data into resources, small, self-contained units that each represent one real-world healthcare concept: a patient, a medication, a condition, a lab result. Older standards moved entire documents or rigid messages, which meant pulling one data point often meant parsing an entire file to find it. FHIR lets a system request exactly the resource it needs through a standard REST API call, the same approach most modern web and mobile apps already use.
That's why a FHIR build moves faster than a legacy integration project tied to older healthcare interoperability standards and protocols: your developers are working with patterns they already know, not a healthcare-specific messaging format they have to learn from scratch.
SMART on FHIR adds an authorization layer on top of FHIR, using OAuth2 to let third-party apps securely connect to an EHR without ever handling a user's login credentials directly. This is what makes building interoperable healthcare platforms realistic at the app level, instead of every new tool requiring its own custom-built integration.
|
Without SMART on FHIR |
With SMART on FHIR |
|---|---|
|
Every app needs a custom integration built and maintained separately |
Apps connect through one standard, reusable authorization layer |
|
Credentials often get shared or duplicated across systems |
OAuth2 keeps user credentials with the EHR, never exposed to the app |
|
Adding a new tool means new engineering work each time |
New apps can plug in through the same connection pattern |
|
Patient and clinician access controls are inconsistent across tools |
Access scopes are defined once and enforced consistently |
If your roadmap includes a patient portal, an app marketplace, or any third-party clinical tool, this is the layer that makes those connections secure and repeatable instead of a one-off project every time.
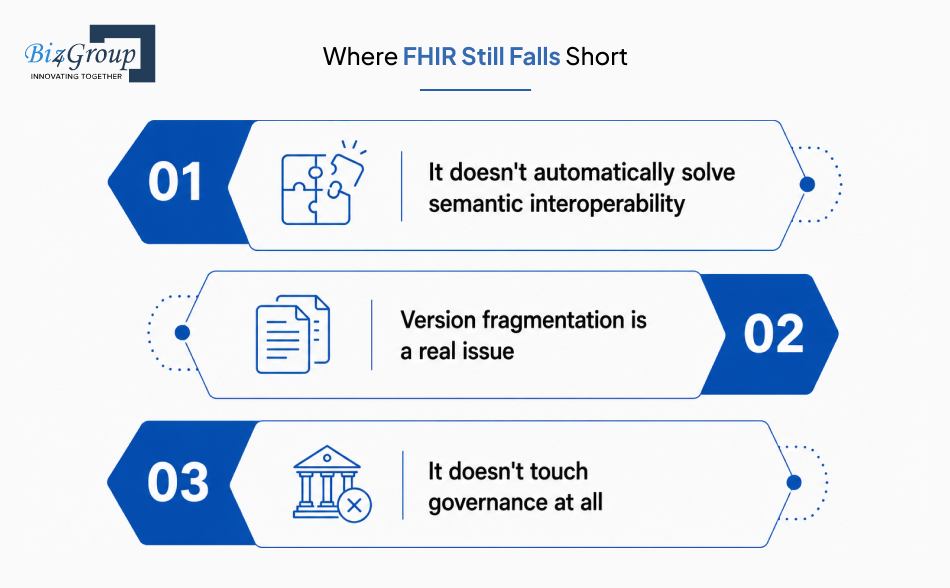
FHIR solves structural interoperability well, but it isn't a complete fix on its own. A few real limits worth knowing before you build around it:
Adopting FHIR gets you a strong technical foundation. It doesn't, on its own, fix what happens when that foundation meets a legacy EHR that was never built to speak this language in the first place, which is exactly where most integration projects actually start running into trouble.
You're running a hospital network with legacy systems sitting alongside newer platforms, and you want to know how to actually achieve interoperability in healthcare across mismatched systems without ripping everything out and starting from scratch.
Here's the direct answer: you don't fix this by replacing everything. You fix it by putting an integration layer between your legacy systems and your modern platforms, standardizing the data that moves through it, and migrating in phases instead of all at once. We've seen this exact approach work for hospital networks carrying the same mix of old and new systems you're dealing with right now. It's what large health systems are doing instead of waiting years for a full rebuild.
But before you build that plan, you need to know exactly where most EHR interoperability in healthcare projects break. That's usually not where leadership expects.
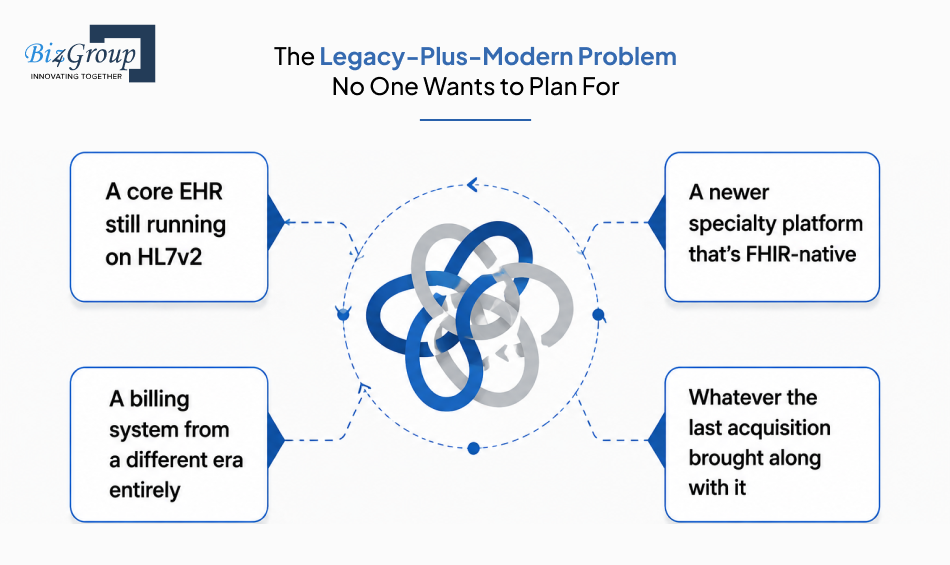
Most hospital networks don't have one outdated system to deal with. They have a mix, often something like:
Each one was built to its own standard, at its own time, by its own vendor. The break doesn't happen because any single system is bad. It happens at the seams between them, where one system sends data in a format the next one was never built to read. Someone ends up manually reconciling the gap by hand. This is the exact starting point for most healthcare system integration and interoperability work, and it's also why a full replacement is rarely the realistic answer.
A small number of vendors dominate the EHR market, and that concentration creates a real incentive problem. Some vendors build APIs that technically check the certification box. In practice, those same APIs can make genuinely open healthcare data interoperability slower and more expensive than it needs to be. If your core EHR vendor isn't actively cooperative about FHIR access, every integration project from there gets harder than the standards alone would suggest. That's a negotiation and contract issue as much as it is a technical one.
A lot of integration work in healthcare gets built to solve one immediate problem rather than the underlying one. A custom point-to-point connection gets built to move a single data feed. It works, so everyone moves on. The real cost shows up later:
Multiply that across a hospital network with a dozen systems, and you get exactly the fragile, expensive mess most CTOs inherit rather than create. It's also exactly why EHR interoperability in healthcare so often gets blamed on "bad systems," when the real cause is years of patchwork fixes stacked on top of each other.
Knowing where these projects break is only half the picture. The other half is what actually causes them to break in the first place, which goes beyond any single vendor or legacy system and into the bigger structural challenges every hospital network is up against.
If your integrations feel held together by duct tape and good intentions, it's time for something sturdier.
Schedule a Strategy Call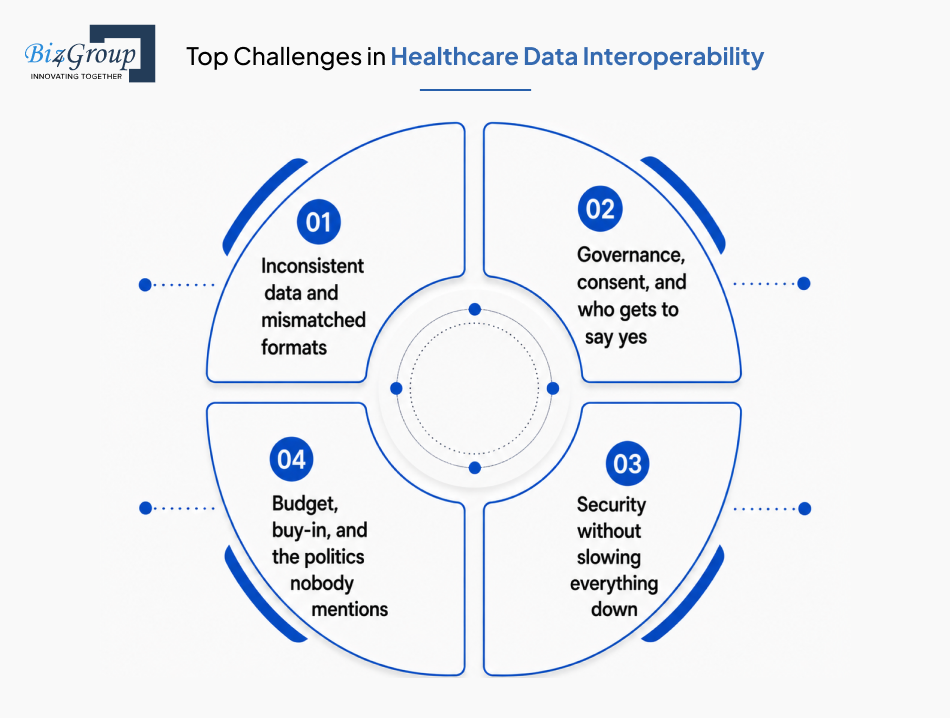
The standards are clear by now, and so is where integration projects tend to break. What's left is the harder question: what's actually blocking healthcare data interoperability inside your organization, and what fixes each one. Here's the honest breakdown, mapped side by side.
|
Challenge |
What's Actually Happening |
How to Fix It |
|---|---|---|
|
Inconsistent data and mismatched formats |
Lab results, diagnoses, and medications arrive coded differently across systems, so nothing lines up without manual reconciliation. |
Map data to standard vocabularies like SNOMED CT, LOINC, and RxNorm, and route everything through an integration layer that enforces a consistent structure before it reaches downstream systems. |
|
Governance, consent, and who gets to say yes |
Data is technically shareable, but nobody has agreed on who's authorized to request it, under what conditions, or how consent is tracked across organizations. |
Build clear data governance policies before scaling exchange, define consent rules upfront, and align them with frameworks like TEFCA, so authorization isn't being figured out case by case. This same governance discipline becomes even more critical once AI tools start touching patient data, which is exactly where AI governance in healthcare needs to be part of the conversation from day one. |
|
Security without slowing everything down |
Tightening access controls to protect PHI often adds friction that slows clinicians down at the point of care. |
Use standards-based authorization like SMART on FHIR, which secures access through OAuth2 without requiring a separate login process for every connected tool, so security and speed stop working against each other. |
|
Budget, buy-in, and the politics nobody mentions |
Leadership sees interoperability as an IT line item rather than a strategic investment, so funding gets deprioritized until a compliance deadline forces the issue. |
Tie the business case to numbers leadership already tracks: reduced administrative hours, fewer duplicate tests, and faster payer reimbursement, so the investment reads as operational, not technical. |
None of these four problems get solved by a single tool or a single vendor swap. They get solved by treating healthcare data interoperability as an ongoing discipline, not a project with a finish line.
That brings us to the part most leadership teams actually want: a real, practical sequence for fixing all of this without tearing existing systems apart to do it.
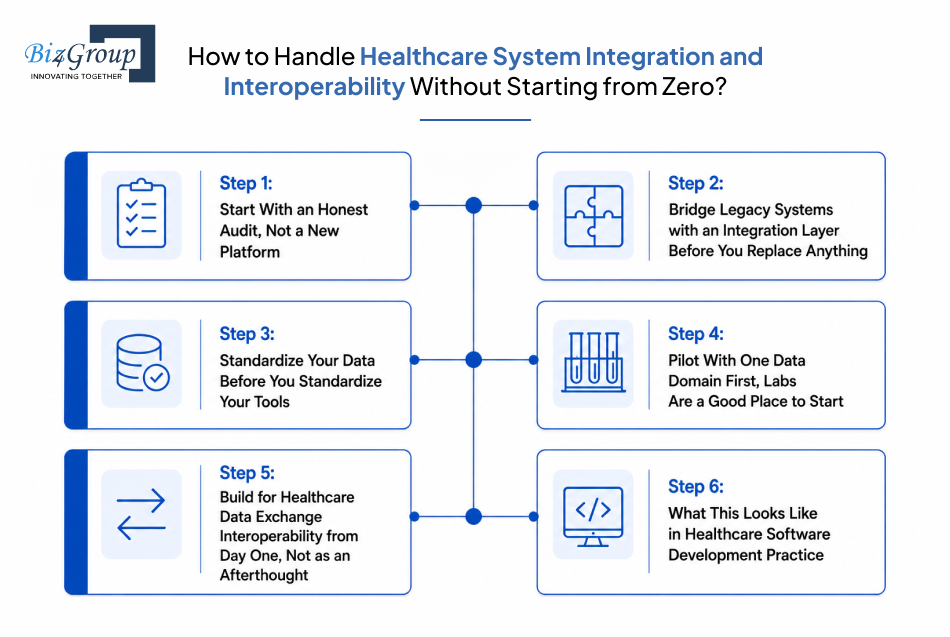
Everything up to this point has been about understanding the problem. This is the part where it actually gets solved. Here's the real sequence for achieving healthcare system integration and interoperability when you're working with a mix of legacy systems and modern platforms, not a greenfield build.
Before any integration work starts, map exactly what you have:
Most networks skip this step and jump straight to buying a new tool. That usually just adds another system to the pile instead of fixing the gaps between the ones already there. This audit is also where you figure out which interoperability level each system is actually stuck at: foundational, structural, semantic, or organizational. The rest of your interoperability in healthcare plan should be built on that, not on assumptions.
An integration engine or FHIR facade sits between your legacy systems and your modern platforms. It translates HL7v2 messages into FHIR resources without touching the underlying systems themselves.
This is the single most practical answer to one question: how do you achieve EHR interoperability in healthcare without ripping everything out? Your legacy EHR keeps running exactly as it does today. The integration layer simply learns to speak both languages. Newer platforms can request data through modern APIs, while older systems keep doing what they've always done.
Buying the same EHR across every facility doesn't fix data interoperability in healthcare if the data inside still uses inconsistent codes and local terminology.
Map everything to shared vocabularies first:
Worry about which platform sits on top later. Tools change every few years. Clean, standardized data outlasts every one of them.
Trying to standardize every data type across every department at once is how these projects stall out.
Pick one domain instead. Lab results are usually the cleanest place to begin. Get that flowing correctly from end to end before expanding anywhere else.
A working pilot does three things at once. It gives your team a proven pattern for building interoperable healthcare platforms at scale. It gives leadership a visible early win. And it surfaces the real integration issues on a small scale, not a network-wide one.
Every new platform you add from this point forward should be evaluated on one thing first: its FHIR readiness and its willingness to support open healthcare data exchange interoperability. Not just its feature list.
A specialty tool with a beautiful interface and a closed, proprietary data format will cost you more in integration work later than it saves you in functionality now. Make interoperability a procurement requirement, not a retrofit.
In practice, interoperability in healthcare software development comes down to three things:
This is also where partnering with a team that's done this specific kind of legacy-to-modern bridging work pays off. The difference between a fragile integration and a durable one usually comes down to experience with exactly this problem. If your team is weighing build versus partner on this, it's worth looking at what a dedicated AI healthcare software development company actually brings to a project like this before committing resources internally.
Follow these six steps in order and you end up with something most hospital networks never expected to have: a system that talks to itself cleanly, without a single legacy platform having to be torn out to get there.
Also Read: AI in Healthcare Explained: 130+ Questions Answered for Healthcare Providers and Innovators

Everything covered so far gets you current. Knowing where things are actually heading is what keeps you ahead of it, because interoperability in healthcare is moving fast right now, and a few shifts already underway will shape how every hospital network operates over the next two years.
FHIR interoperability standards have crossed a real tipping point: Firely's State of FHIR report found that 71% of organizations now use FHIR in active, operational workflows, a sharp jump from the year before. The shift underway in 2026 is that FHIR compatibility is becoming a prerequisite for new vendor contracts and technology partnerships, not just a nice-to-have feature on an EHR's spec sheet.
Industry leaders expect 2026 to be the most significant year of interoperability in healthcare progress the industry has seen, driven largely by CMS mandates on health plans. By the end of 2026, most health plans are expected to share data downstream to a member's new health plan and pull data from a member's former plan, with providers able to retrieve full claims and clinical data directly through on-demand FHIR APIs. That shifts prior authorization and care coordination away from manual, fax-driven processes for good.
Healthcare data used to move on a schedule: nightly batch jobs, periodic syncs, end-of-shift updates. That model is giving way to event-driven architecture, where data from connected devices, telehealth visits, and clinical systems triggers an immediate response instead of sitting in a queue for later review. This shift matters because healthcare data exchange interoperability is no longer just about whether data eventually arrives, it's about whether it arrives fast enough to change a clinical decision in the moment.
Clean, standardized healthcare data interoperability is what makes AI in healthcare useful instead of risky. A model trained on incomplete or mismatched records produces incomplete or mismatched recommendations, no matter how advanced the model itself is. This is exactly why the networks furthest ahead on EHR interoperability in healthcare are also the ones getting real value out of automation, whether that's intelligent triage, predictive staffing, or AI healthcare workflow automation handling the repetitive coordination work that used to eat up staff hours.
As prior authorization and patient access rules take effect, organizations that haven't invested in clean coding and terminology mapping are running into data fragmentation and inconsistent code sets at exactly the moment they need data interoperability in healthcare to flow. Industry voices are already pointing to FHIR-based terminology services as the next layer of investment, since normalizing clinical data and maintaining consistent mapping across systems is what separates organizations actually getting value from healthcare system integration and interoperability versus those just technically compliant with it.
None of these trends are abstract. Each one is already reshaping vendor contracts, payer relationships, and IT roadmaps right now, and they're worth tracking alongside the broader healthcare IT trends shaping the industry's direction more broadly.
Everything in this guide reflects how we actually approach interoperability in healthcare with our own clients, not theory borrowed from somewhere else.
We've spent over 20 years building software for healthcare organizations, and more than 100 of our completed projects have been AI-powered, data-driven healthcare initiatives. That work has generated over $500 million in revenue for our clients, and a meaningful share of it has involved exactly the problem this guide is built around: getting legacy systems and modern platforms to actually achieve real healthcare data interoperability.
Our engineering teams work directly with FHIR interoperability standards, HL7, DICOM, X12, and SMART on FHIR as part of our standard healthcare stack, alongside integration tools like Mirth Connect and Redox API that are built specifically for bridging older messaging formats with modern, FHIR-based exchange. That's the same integration-layer approach we walked through earlier in this guide for achieving healthcare system integration and interoperability, applied in real client environments rather than as a hypothetical.
A few things shape how we handle this work in practice:
If you're weighing whether to integrate healthcare platforms with AI EHRs or rebuild around a new core system, that decision usually comes down to exactly the kind of audit and phased approach covered earlier in this guide, the one built for building interoperable healthcare platforms without a disruptive rebuild. We've documented how that's played out for real clients in our top AI healthcare case studies, covering the kind of legacy modernization, EHR integration, and AI-enabled workflow work that hospital networks and health-tech teams bring to us most often.
If your team is at the point of mapping out what healthcare data exchange interoperability looks like for your specific systems, that's a conversation we're set up to have, with the same engineers who'd actually be doing the integration work sitting in the room.
No rip-and-replace required. Just a team that's done this before and knows exactly where it usually breaks.
Start the ConversationGetting interoperability in healthcare right isn't about replacing everything you've built. It's about giving your legacy systems and modern platforms a common language, standardizing your healthcare data interoperability efforts, and rolling out healthcare system integration and interoperability in phases that don't put patient care at risk along the way.
The organizations that get ahead of this aren't the ones with the newest systems. They're the ones with a clear plan for making old and new work together. It's also why an 85% client retention rate and a 4.9-star rating on Clutch follow the kind of work Biz4Group does on exactly these problems, the kind hospital networks and health-tech teams come back for once the first phase actually works.
So, ready to stop playing phone tag between your own systems? Let's talk.
Interoperability in healthcare is the ability for different systems, EHRs, labs, pharmacies, and hospitals, to exchange patient data accurately and securely, so the information is usable the moment it arrives instead of requiring manual entry or a phone call to confirm.
For a hospital network running multiple facilities or systems, why is interoperability important in healthcare comes down to patient safety, reduced duplicate testing, faster care coordination, lower administrative costs, and an easier path through CMS and ONC compliance, since fragmented data slows down every one of those areas at once.
The core healthcare interoperability standards and protocols are HL7v2 for legacy messaging, FHIR R4 for modern API-based exchange, C-CDA for clinical documents, and X12 for administrative and claims transactions, with USCDI and TEFCA governing what data gets shared and under what rules.
FHIR interoperability standards use REST APIs and JSON to move discrete, reusable data resources, while HL7v2 moves rigid messages with so many optional fields that two compliant systems often still need custom mapping to understand each other.
Yes. EHR interoperability in healthcare can be achieved by placing an integration engine or FHIR facade between legacy and modern systems, so the legacy EHR keeps running as is while the integration layer translates data between formats.
Healthcare data interoperability refers to how data itself is structured, coded, and exchanged across any system, while EHR interoperability refers specifically to how electronic health record platforms connect and share that data with each other.
The cost of healthcare system integration and interoperability depends on the number of systems involved, the standards already in place, and whether the project starts with legacy systems or a clean build, which is why most organizations start with an audit before getting a real estimate.

Our website require some cookies to function properly. Read our privacy policy to know more.